AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/IJBR-2021/023
*Corresponding Author: Abdul Rauf Alhassan, Department of Surgery, Tamale Teaching Hospital, P.O. Box TL 16; Tamale Ghana
Citation: Abdul R. Alhassan (2021) Under-five Mortality in Ghana: Prevalence and Socioeconomic Predictors 1(6); International Journal of Biomed Research. 1(6); DOI:10.31579/IJBR-2021/023
Copyright: © 2021, Abdul Rauf Alhassan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 June 2021 | Accepted: 10 July 2021 | Published: 07 September 2021
Keywords: ghana; mortality; predictors; under-five;
Background: Under-five mortality remains serious public health importance and contributes to the estimates of life expectancy of any country at birth, which is a key health indicator.
Aim: This study aimed to identify the prevalence and socioeconomic predictors of under-five mortality in Ghana.
Method: The study design was a descriptive cross-sectional survey relying on data from Ghana Multiple Indicator Cluster Survey (MICS) 2017/18. The analysis was done using SPSS version 20 (IBM Corp., 2011, and NY).
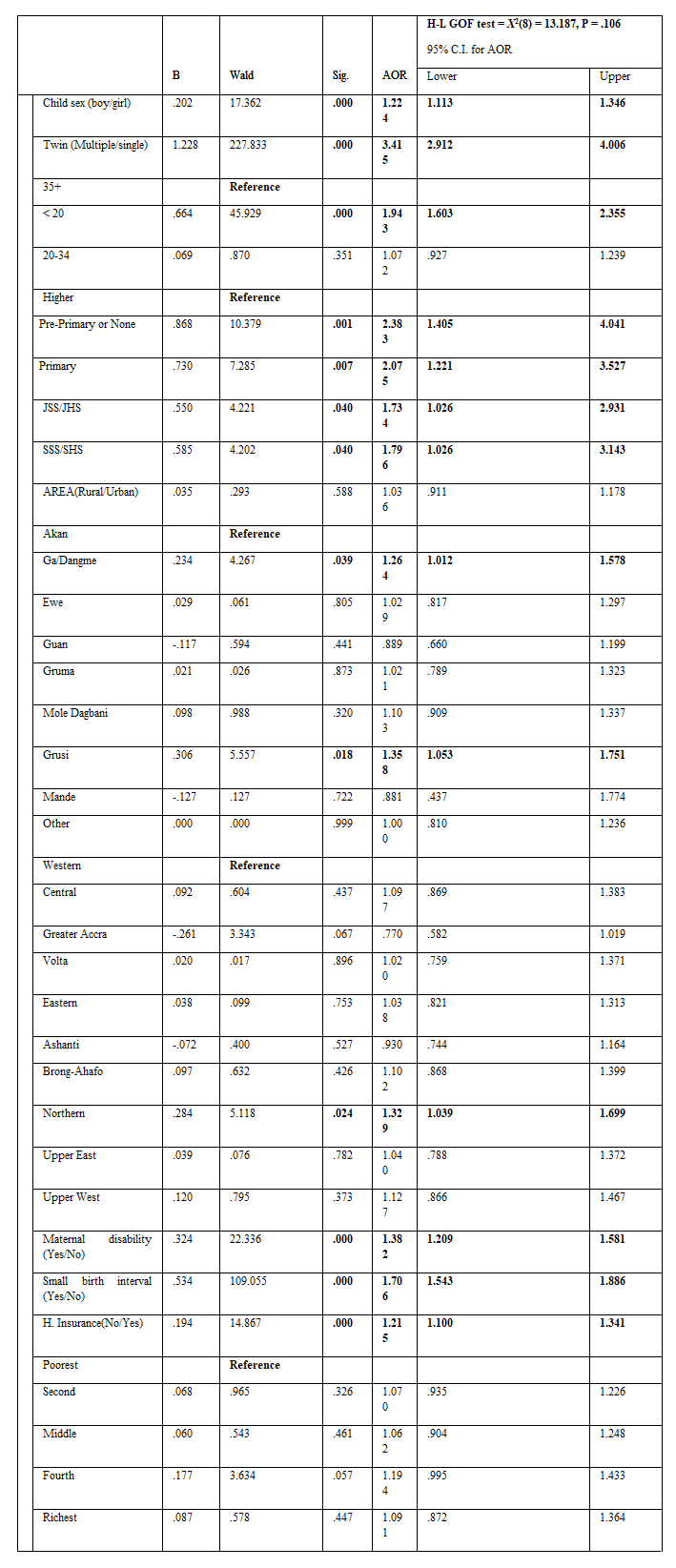
Results: In this study the prevalence of under-five mortality recorded was 8.4% and socioeconomic predictor factors were: male sex of child (AOR = 1.2, 95% C.I. = 1.11 – 1.35), maternal age, < 20 years (AOR = 1.9, 95% C.I. = 1.60 - 2.36), education level, No education (AOR = 2.4, 95% C.I. = 1.41 – 4.04), Primary (AOR = 2.1, 95% C.I. = 1.22 – 4.04), JSS/JHS/Middle (AOR = 1.7, 95% C.I. = 1.03 – 2.93), SSS/SHS (AOR = 1.8, 95% C.I. = 1.03 – 3.14), Ethnicity, Ga/ Dangme (AOR = 1.3, 95% C.I. = 1.01 – 1.58) and Grusi (AOR = 1.4, 95% C.I. = 1.05 – 1.75), region Northern/Western region (AOR = 1.3, 95% C.I. = 1.04 – 1.70), mother with functional disabilty (AOR = 1.4, 95% C.I. = 1.21 – 1.58), short birth interval (AOR = 1.71, 95% C.I. = 1.54 – 1.89) and no health insurance (AOR = 1.22, 95% C.I. = 1.10 – 1.34).
Conclusion:
prevalence of under-five mortality was high and socioeconomic predictors factors identified were: maternal age, educational level, ethnicity, region, functional disability, short birth interval, and health insurance status
Under-five mortality remains serious public health importance. Under-five contributes to the estimates of life expectancy of any country at birth, which is a key health indicator [1]. In 2013 UNICEF report had it that each year 6.6 million children die, and this translated into 546000 per month, for week 125000, for a day 18000, and 12 deaths for every minute [2]. This means each time one takes a breath a child dies. However, in recent times the estimate of under-five mortality has declined from 12.6 million (in 1990) to 5.6 million (in 2016) [3]. There has a great variation of under-five mortality rates across regions and countries [4,5].
In sub-Saharan Africa, the estimates of under-mortality remain the highest as compared to the global community. The under-five mortality estimate for sub-Saharan in 2016 was 79 per 1000 live births and this figure implies that 1 out of 13 children dies before the five birth date. Meanwhile, in the highly developed nations, the estimate is 15 times higher and 20 times higher for countries like New Zealand and Australia [3,6].
In Ghana, equally of serious public health significance is the rates of under-mortality and also the decline in rates has been so slow and not satisfactory since 1988 to 2003 and the current estimate according to UNICEF if 74 per 1000 live births [2]. Also, world data alas has it that, in 2019, the under-five mortality estimate for Ghana was 46.2 deaths per 1,000 live births. The child mortality estimate of Ghana declined slowly from 202.3 deaths per 1,000 live births in 1970 to 46.2 deaths per 1,000 live births in 2019 [7]. However, there exist variations with regards to under-five mortality estimates among the regions of Ghana, with a lower rate for the better resource south regions as compared to the deprived regions of northern Ghana [8].
About sixty percent of under-five mortalities are preventable and factors implicated in the cause of death are unsafe water, malnutrition, poor health care, major services, and lack of education. [6]. WHO 2015 global health estimates have it that, the most significant causes of under-five mortality are; preterm complication (17%), pneumonia (15%), birth asphyxia (11%), diarrhea (9%), malaria (7%), congenital anomalies (7%) and neonatal infections (15%) [9].
Socioeconomic, demographic, and biological factors are the main factors responsible for under-five mortality. Socioeconomic factors largely result in the endogeneity of child deaths, for example, uvula cutting, milk teeth extraction, female genital mutilation, and eyebrow incision after birth which is always closely associated with socio-economic and cultural practice. Demographic factors affect both endogenous and exogenous deaths, like problems at birth which are difficult to prevent and control, and exogenous deaths which can be prevented by public health measures, immunization, and antibiotic treatment. Biological factors mainly refer to the mother’s fertility information and the total number of children born which are concerned at the family level rather than children [10,11].
Studies in sub-Saharan Africa identified socioeconomic factors as predictors of under-five mortality [12,13]. In an Ethiopian study by Woldeamanuel, Children born to mothers with no education were likely about three times to die before their five birthday. Those with short birth spacing were also likely about two times to die before age five years. Also, babies with birth orders of five and above were likely to die before age of five years [12]. In Zewudie et al. study, rural residency, multiple, male gender, first birth order, and breastfeeding predicted under-five mortality in Ethiopia [13].
In Ghana, multiple birth and geographical location predicted under-five mortality, and the female sex of a child and maternal education decreased the odds of under-five mortality [14]. In another study in Northern Ghana, maternal age a birth, mother education level, and household socioeconomic status were significantly related to under-five mortality [15]. There is little knowledge of studies with regards to Ghana's national wide studies on predictors of under-five mortality in Ghana, hence this study aimed to identify the prevalence and socioeconomic predictors of under-five mortality in Ghana.
A descriptive cross-sectional survey design was used using Ghana Multiple Indicator Cluster Survey (MICS) 2017/18 data. Ghana Statistical Service conducted this survey from October 2017 to January 2018 in collaboration with the Ministry of Health, Ministry of Education, Ministry of Sanitation and Water Resources, Ministry of Gender, Children and Social Protection, Ghana Health Service, and the Ghana Education Service as part of the Global MICS Programme. Technical support was provided by the United Nations Children’s Fund (UNICEF), with government funding and financial support of UNICEF, KOICA, UNDP, USAID, and the World Bank through the Statistics for Results Facility – Catalytic Fund (SRF-CF).
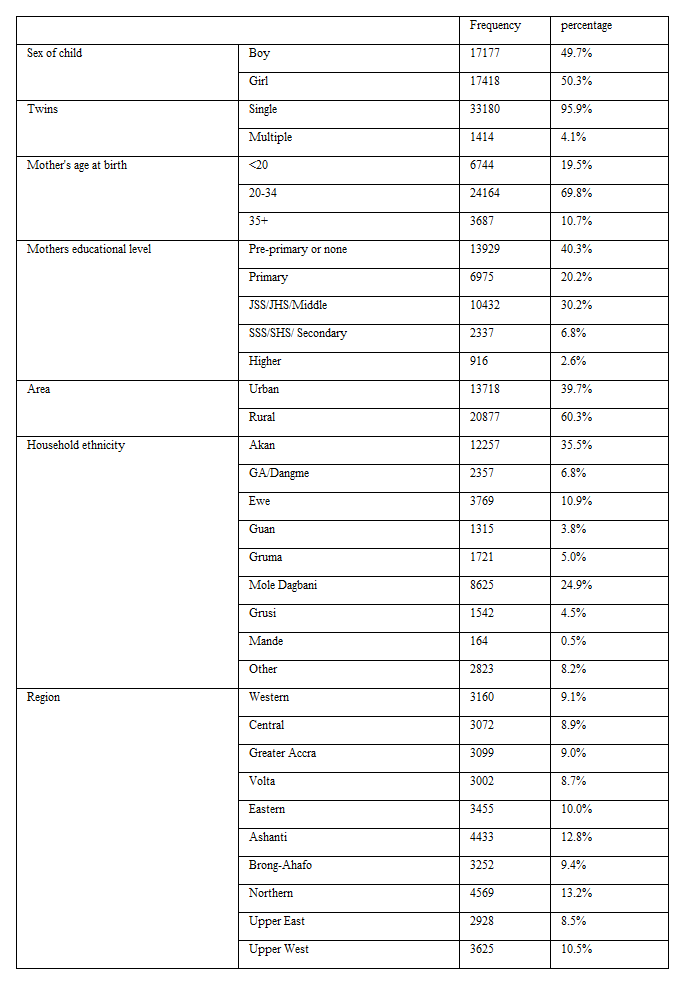
The sampling frame assumed was from the Ghana 2010 Population and Housing Census (PHC). This encompassed women (34595) aged 15-49 years with a history of childbirth who were permanent occupants of selected households or visitors who stayed in selected households the night before the survey.
Statistical analysis was accomplished by using SPSS version 20 (IBM Corp., 2011, and NY). Categorical variables results were presented using frequencies and percentages using tables. The association between dependent and independent variables was done using chi-square. The binary logistics regression model was used to identify predictor variables of the main outcome variable (under-five mortality). Statistical significance was set at a p-value of < 0>
Dependent variable: The main outcome variable was under-five mortality.
Independent variables: The studied socioeconomic characteristics of the study.
The survey employed a multistage sampling methodology. Clusters that represented sampling units were randomly selected in the first stage using and the 2010 Population and Housing Census of Ghana were used as the census frame to select the clusters. Stratification was used to select the place of residence (i.e., urban stratum or rural stratum). The clusters were randomly selected during the first stage. In the second stage, systematic sampling was applied for households’ selection. The field data collection instrument included 6 questionnaires: Household questionnaire, Water Quality Testing Questionnaire, Questionnaire for Individual Women, Questionnaire for Individual Men, Questionnaire for Children under Five, and Questionnaire for Children Age 5–17. However, for this study, data used was from the Questionnaire for Children under five which was administered to the randomly selected child's mother or caretaker living in the household. Details of the methodology used for the survey are available with Ghana Health Service [18].
The nationwide prevalence of under-five mortality recorded in this study was 8.4%, highest under-five mortality rates above the national average were recorded in the northern regions of Ghana, Northern region (11.7%), Upper West (10.4%), and Upper East (9.3%) and the lowest rate was recorded in Greater Accra region.
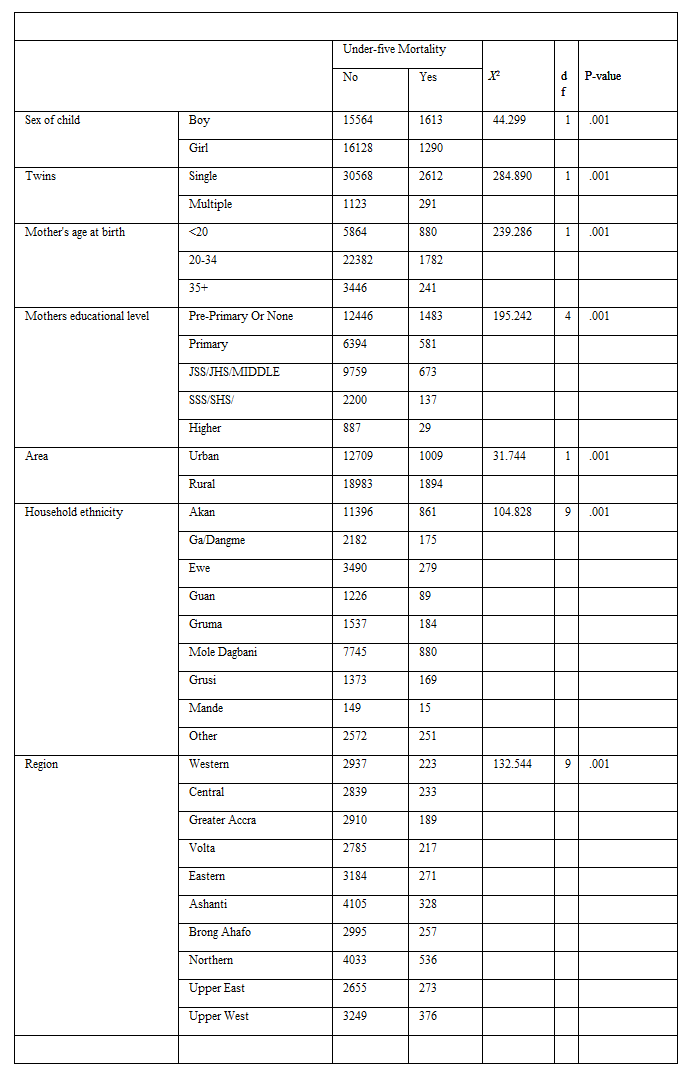
Factor associated with under-five mortality in Ghana
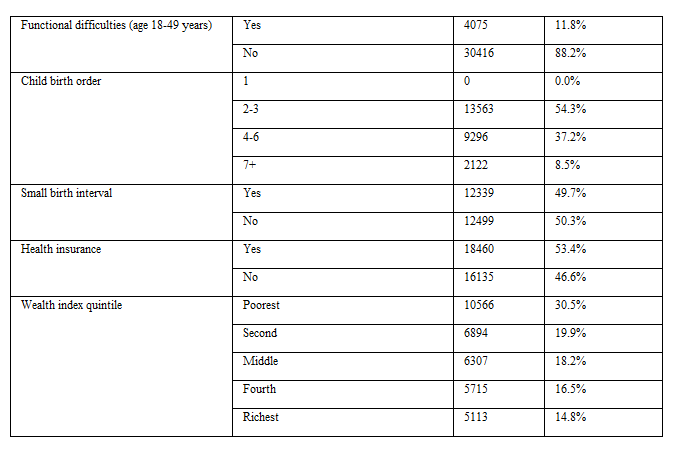
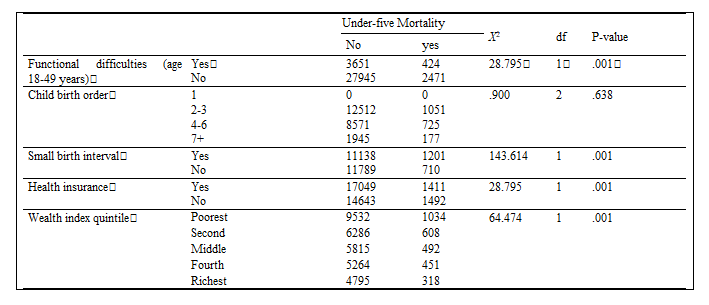
The factors associated with under-five mortality in this current study were: child sex, twins, mother’s age at birth, mother education, area, household ethnicity, region, maternal disability status, small birth interval, health insurance status, and wealth index status. However, childbirth order was significantly associated with under-five mortality (Table 3). With the trends of death in terms of age at death, the chance of death decreased as the child age increased. Most of the deaths were before the age of two years (figure 1).
Predictors of under-five mortality in Ghana
Binary logistics analysis identified sex of the child as a predictor of under-five mortality, male children were likely about 1.2 times to experience under-five mortality as compared to female children (AOR = 1.2, 95% C.I. = 1.11 – 1.35). Lower age of mother ( below 20 years) at birth predicted child under-five mortality, < 20 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>p-value was more than 0.05, H-L GOF test (X2(8) = 13.187, P=0.106), hence the model fits the study data (Table 5).
The nationwide prevalence of under-five mortality recorded in this study was 8.4%, the prevalence is higher when compared with the earlier prevalence in Ghana [14]. This recorded prevalence is not good when related to progress made according to a study, the Child mortality estimate of Ghana declined slowly from 202.3 deaths per 1,000 live births in 1970 to 46.2 deaths per 1,000 live births (4.6%) in 2019 [7]. Also, the prevalence is higher when compared with the earlier prevalence in sub-Saharan Africa [3]. Most of the deaths were before the age of two years. The highest under-five mortality rates above the national average were recorded in the northern regions of Ghana, Northern region (11.7%), Upper West (10.4%), and Upper East (9.3%) and the lowest rate was recorded in the Greater Accra region. This is a confirmation that in Ghana, geographical location predicted under-five mortality [14]. There exist variations with regards to under-five mortality estimates among the regions of Ghana, with a lower rate for the better resource south regions as compared to the deprived regions of northern Ghana [8].
Binary logistics analysis identified the sex of the child as a predictor of under-five mortality, male children were likely about 1.2 times to experience under-five mortality as compared to female children. In a similar study, the odds of child survival increased with the female sex [14].
Lower age of mother ( below 20 years) at birth predicted child under-five mortality, < 20>
Also, children born from mothers with an education level less than tertiary (higher) predicted under-five mortality. Meaning lower maternal educational status is a predictive factor of under-five mortality in Ghana per this current study and this confirms earlier studies [12,14, 15].
Additionally, ethnicity is associated with variations in health beliefs and behaviors, social cohesion, and therefore in the dissemination of health information. As a basis of identification, for political reasons, ethnicity can be related to uneven admittance to socioeconomic opportunities and public goods. In this current study children from Ga/ Dangme ethnic background were likely about 1.3 times to experience death before their five days as compared to those from Akan ethnic background, and in the same vein children from Grusi ethnic background were like about 1.4 times to experience under-five mortality as compared to those from Akan background. Also, a study in Africa indicated that the largest ethnic group did not have the lowest U5MR in any of the countries studied [17]. Those from the northern region were like to suffer under-five mortality as compared to those from the Western region. In a similar Ghana study, the northern region predicted under-five mortality [14].
Furthermore, children from mothers with functional disabilities were likely 1.4 times to suffer under-five mortality. Mothers with a functional disability may less supportive of their babies compared to those without a functional disability. And children with short birth intervals were more likely 71% to suffer under-five mortality than those without short birth intervals. In line with a similar study, short birth spacing 1 to 18 months birth intervals predicted under-five mortality by the extra chance of 102% [12].
Finally, those without health insurance were more likely about 22% to suffer under-five mortality than those with health insurance. Access to health is increased with health insurance and health insurance status is influences by economic status. In the northern Ghana study, a mother’s household socioeconomic status was significantly related to child mortality [15].
This study was not without limitations, not all variables like religion, duration of breastfeeding, etc. were explored. Which when explored will help throw more light on the research question.Conclusion
The prevalence of under-five mortality in this study was high and the socio-demographic factors that predicted under-five mortality included: maternal age, ethnicity, and educational level, region, not having health insurance, maternal functional disability, and small birth interval. This high prevalence indicates that the progress made in the previous years is affected hence the need for review action to bring back the prevalence towards reducing trend.
Alhassan, AR designed this study and the principal author of this manuscript. From conceptualization to final draft of the manuscript.
All data related to the findings of this study are available from the UNICEF / MICS website (https://mics.unicef.org) upon request.
There is no conflict of interest with this submission.
Funding for this study was completed by authors without any external funding.
Not required.
The MICS team of UNICEF approved the protocol for the use of the Ghana Multiple Indicator Cluster Survey 2017/18 dataset for this study. Ethical approval was not necessary for this study because it involved a secondary analysis of a dataset without publicity to the identity of the participants and their households.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.