AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1045/008
*Corresponding Author: Shereen Abdelghaffar, Professor of Pediatrics, Pediatric Endocrinology and Diabetes , Ethiopia.
Citation: Shereen Abdelghaffar, Mohamed A Ghoneim, Mohamed Adel el-Masry, Ashraf F Nabhan, Ashraf Anas Zytoon. Primary Congenital Hypothyroidism: Pharmacokinetics of Levothyroxine for the Treatment of Hypothyroidism. J. Endocrinology and Disorders. Doi:10.31579/2640-1045/008
Copyright: © 2017. Shereen Abdelghaffar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 June 2017 | Accepted: 19 July 2017 | Published: 10 August 2017
Keywords: Neonatal screening, congenital hypothyroidism, iodine deficiency.
Primary congenital hypothyroidism (CH) is a condition that affects the body's thyroid gland, a small organ in the lower neck. People with CH are unable to produce enough thyroid hormone, a chemical that is essential for healthy growth and development.
If left untreated, CH can cause sluggishness, slow growth, and learning delays. However, if detected early and treatment is begun, individuals with CH often can lead healthy lives.
Most neonates born with CH have normal appearance and no detectable physical signs. Hypothyroidism in the newborn period is almost always overlooked, and delayed diagnosis leads to the most severe outcome of CH, mental retardation, emphasizing the importance of NS. Blood spot thyroid stimulating hormone (TSH) or thyroxine (T4) or both can be used for CH screening. The latter is more sensitive but not cost-effective, so screening by TSH or T4 is used in different programs around the world. TSH screening was shown to be more specific in the diagnosis of CH. T4 screening is more sensitive in detecting especially those newborns with rare hypothalamic-pituitary-hypothyroidism, but it is less specific with a high frequency of false positives mainly in low birth weight and premature infants. The time at which the sample is taken may vary. In the majority of the centers, blood is obtained from a heel prick after 24 hours of age to minimize the false positive high TSH due to the physiological neonatal TSH surge that elevates TSH levels and causes dynamic T4 and T3 changes in the first 1 or 2 days after birth. Early discharge of mothers postpartum has increased the ratio of false positive TSH elevations. Although transient hypothyroidism may occur frequently, all these infants should be treated as having CH for the first 3 years of life, taking into account the risk of mental retardation. A reevaluation after 3 years is needed in such patients. The goal of initial therapy in CH is to minimize neonatal central nervous system exposure to hypothyroidism by normalizing thyroid function, as rapidly as possible.
As is often the case with older drugs, the pharmacokinetics of levothyroxine is often under-appreciated or misunderstood and many factors influence the optimal dosing of levothyroxine.
Congenital hypothyroidism (CH) is the most common congenital endocrine disorder in childhood and also is one of the most common preventable causes of mental retardation. After making diagnosis if the treatment is started within in a few weeks of birth, neurodevelopmental outcome is generally normal. The clinical features of congenital hypothyroidism are often subtle and many newborn infants remain undiagnosed at birth. This is due in part to passage of maternal thyroid hormone across the placenta providing a protective effect, especially to the fetal brain and masking the clinical signs. Also, even the most common forms of CH have some moderately functioning residual thyroid tissue making clinical diagnosis difficult. Within few weeks of birth as hypothyroxinemia progresses clinical signs and symptoms of hypothyroidism become more obvious and put neonatal brain at risk of irreversible injury. Because of this danger, it is important to start treatment as soon as possible after birth. For all of the above reasons, screening has become the best way to detect infants with CH in many parts of the world. Pilot screening programs for CH were developed in Quebec, Canada and Pittsburgh, Pennsylvania in 1974 and have now been established in Western Europe, North America, Japan, Australia and parts of Eastern Europe, Asia, South America and Central America. As Indian data are lacking, In North America, more than 5 million newborns are screened and approximately 1400 infants with CH are detected annually.
Newborn screening (NS) for CH is one of the major achievements of preventive medicine. Although since 1972 the problem of CH has been resolved in developed countries by the implementation of NS, the same cannot be said for developing countries that still have no NS programs for CH. Since diagnosis based on clinical findings is delayed in most instances because of few symptoms and signs, hypothyroidism in the newborn period is almost always overlooked, and delayed diagnosis leads to the most severe outcome of CH, namely, mental retardation. In a Danish study conducted on infants born between 1970 and 1975, it was emphasized that only 10% of the affected infants were diagnosed within the first month of life, 35% within 3 months, and 70% within the first year. In the remainder of the infants, the diagnosis was delayed to the 3rd and 4th years of life. In a retrospective analysis of 1000 cases of CH from Turkey, the mean age at diagnosis was reported to be 49 months, and only 3.1% of cases were diagnosed within the first month, while 55.4% were diagnosed after 2 years of age.
Epidemiology
The overall incidence of CH ranges from 1 in 3000 to 1 in 4000 newborn infants. The incidence of CH is higher in Hispanic and Asian individuals and lower in black individuals. There is a 2:1 greater incidence in females compared with males and there is an increased risk in infants with Down's syndrome. In India, the prevalence has been reported to be 1 in 2640 in screening 40,000 newborn. In 2007, Harris and Pass reported that the incidence (birth prevalence) of CH detected by newborn screening programs in the United States had nearly doubled over the previous two decades, increasing from 1:3985 (in 1987) to 1:2273 (in 2002).
Etiology
In the majority of patients, CH is caused by an abnormal development of the thyroid gland (thyroid dysgenesis) which is usually a sporadic disorder and accounts for 85% of cases. It presents in three major forms i.e. thyroid ectopy, athyreosis and thyroid hypoplasia. Thyroid ectopy accounts for two thirds of cases of thyroid dysgenesis and is twice more common in females. The exact etiology of thyroid dysgenesis is not known. However; mutations in transcription factor genes that regulate thyroid gland development [thyroid transcription factor 2 (TTF-2), NKX2.1 (also termed TTF-1) or PAX-8] would explain these defects. But, only 2% of cases with thyroid dysgenesis are found to have such genetic mutations.
Diagnostic evaluation
In countries where newborn screening programs take place, all infants with CH are diagnosed after detection by newborn screening tests. However, of the worldwide birth population of 127 million, only 25% of babies are invited for screening for CH. For the remaining 75% infants, particularly concentrated in developing countries, clinical suspicion of hypothyroid leads to thyroid function evaluation.
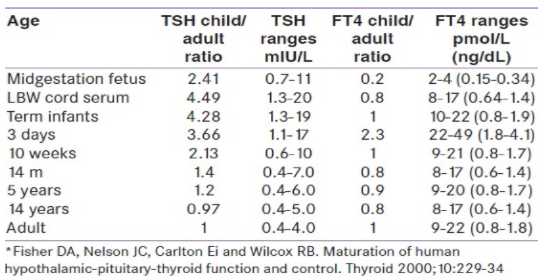
The ideal time to obtain the blood spot is 3-5 days after birth to minimize the false positive high TSH values due to the physiological neonatal TSH surge that elevates TSH levels and causes dynamic T4 and total triiodothyronine (T3) changes in the first 1 or 2 days after birth. Early discharge of mothers postpartum has increased the ratio of false positive TSH elevations from 3:1 to 5:1. The difficulty in screening for CH using cord blood samples is with the handling and transporting the samples, making it an impractical method for mass screening.
In some laboratories, the threshold cut-off is adjusted based on the age of the infant when the blood spot is obtained. The cutoff for reporting an elevated TSH is a level above 20 to 25 mU/mL in most screening programs. Whichever method is used, babies whose initial TSH is >50 mU/mL are most likely to have permanent CH, whereas a TSH level between 20 and 49 mU/mL is frequently a false positive or represents transient hypothyroidism. Transient CH is particularly common in premature infants in borderline iodine-deficient areas.
Newborn thyroid screening protocols
Newborn thyroid screening tests are carried out before discharge from hospital, optimally between 2 and 5 days of age. Specimen collected before 48 h of age may lead to false positive result. Screening of very sick newborn or after blood transfusion may lead to false negative result.
In a critically ill infant or preterm neonate, or in case of home delivery, blood sample should be collected by 7 days of age. Capillary blood samples from heel prick are placed on circles of specialize filter paper, dried at room temperature, then sent to a centralized laboratory. Some programs obtain a routine second specimen between 2 and 6 week of age. The additional incidence of CH based on a second screening at 2 weeks of age is approximately 1 in 30 000.
Earlier for screening of newborn for CH, most programs undertook an initial T4 test, followed by TSH testing if the T4 value falls under a cut off limit. With increasing accuracy of TSH assays on small blood volumes, many screening programs now have switched to an initial TSH test approach to detect CH. Each program should develop its own T4 and TSH cut off for test result. Both methods allow detection of the majority of infants with CH but each approach has its own advantages and disadvantages. The initial T4 then follow up TSH approach will detect some cases of secondary or central hypothyroidism and infant with "delayed TSH elevation". On other hand initial TSH approach will detect mild or subclinical forms of hypothyroidism. Generally, if the screening T4 value is below the 10 th percentile of cut off and/or the TSH is greater than 30mU/liter (15mU/liter whole blood), an infant should be recalled for confirmatory serum testing. In cases with "intermediate results," e.g. low T4 but TSH below cutoff, a program may recommend that a repeat heel prick screening specimen be collected and sent for analysis.
Confirmatory serum thyroid testing
Diagnosis and treatment should not be based on screening test results alone. Neonates with abnormal thyroid screening tests should be recalled immediately for examination and a venipuncture blood sample should be drawn for confirmatory serum testing. Confirmatory serum should be tested for TSH and free T4, or total T4 combined with some measure of binding proteins such as a T3 resin uptake. Serum TSH and T4 undergo dynamic changes in the first weeks of life; it is important to compare the serum results with age-related reference values. [21] In the first few days of life, serum TSH can be as high as 39mU/L, because of the TSH surge that is normally seen after birth. Most confirmatory serum tests are obtained within one to two weeks of age, when the upper TSH range has fallen to an approximately 10mU/liter. Although levels of all hormones are higher at 1-4 days of age, by 2-4 weeks of age they have fallen closer to the levels typically seen in infancy.
Low T4 and elevated TSH values
A low total T4 or free T4 level in the presence of an elevated serum TSH level confirms the diagnosis of primary hypothyroidism. Replacement therapy with levothyroxine (L-T4) should be initiated as soon as confirmatory tests have been drawn before the results of the confirmatory tests are available. Infant with an elevated serum TSH level and a normal free T4 or total T4 is consistent with the diagnosis of subclinical hypothyroidism.
Normal T4 and elevated TSH values
Infant with an elevated serum TSH level and a normal free T4 or total T4 have either a transient or permanent thyroid abnormality or delayed maturation of the hypothalamic-pituitary axis. There is controversy regarding the need for L-T4 therapy in this setting. As TSH concentration is the most sensitive indicator of hypothalamic-pituitary- thyroid axis. A persistent basal TSH concentration higher than 10mU/L (after the first 2 weeks of age) is considered to be abnormal. Therefore, if the TSH elevation persists, the infant should be treated. If such infants are not treated, measurement of FT4 and TSH should be repeated at 2 and 4 weeks and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized.
Low T4 and normal TSH values
The low T4 with normal TSH profile may result from hypothalamic immaturity particularly in preterm infants, during illness, in central hypothyroidism or in primary hypothyroidism and delayed TSH elevation. There are no clear-cut guidelines regarding follow-up of such patient, to follow-up with serial filter-paper screening tests until the T4 value becomes normal, or to request a second blood sample for measurement of FT4 and TSH. Most infants with low T4 and normal TSH have normal FT4 values and the subsequent thyroid function test results are normal. Treatment of these infants (with the exception of those with central hypothyroidism) with L-T4 has not yet been shown to be beneficial.
Diagnostic studies to determine an underlying etiology
once the diagnosis of CH is confirmed, treatment should never be delayed pending the determination of etiology. Additional studies to determine the underlying cause may be done. But these studies are complimentary as these diagnostic studies do not alter treatment decision.
Pharmacokinetics of Levothyroxin
Levothyroxine (l-thyroxine) tablet is crushed and mixed with breast milk, formula or water and resultant suspension is squirted into cheek pad or can put on open nipple for infant to feed. Various substances interfere Levothyroxine (l-thyroxine) absorption through gut, such as calcium and iron preparation, soy protein formula, sucralfate, aluminium hydroxide and cholestyramine should not be given together. Although, recommendation is to take Levothyroxine (l-thyroxine) empty stomach but for infant it may not be possible.
Dosages
The goal of therapy is to normalize T4 within 2 weeks and TSH within one month. In one study infants who took longer than 2 weeks to normalize thyroid function had significantly lower cognitive, attention and achievement scores than those who achievement scores than those who achieved normal thyroid function at 1 or 2 weeks of treatment. As an optimal neurological development depends on both adequacy and timing of treatment, American academy of pediatrics and European society of pediatric endocrinology recommend 10-15 μgm/kg/day as initial dose. Studies show that this dose normalizes serum T4 within 3 days and TSH within 2-4 weeks. Initial LT4 dose and rapid normalization of serum T4 are critical to the optimal neurodevelopmental outcome. In severe CH, it is important to start higher initial dose of the recommended range to achieve these goals. In one study infants who started on higher initial doses 50μgm had full-scale IQ scores 11 points higher than those started on lower initial doses 37.5 μgm.
Target concentrations
Guidelines of American academy of pediatrics and European society for pediatric endocrinology recommend that T4 concentrations should be kept in the upper half of reference range. Target values for T4 are 10-16 μgm/dl; FT4 1.4-2.3ng/dl and TSH <5 μU/dl (optimally 0.5-2.0 μU/dl) for first 3 years of life. Thereafter, T4 should be kept in the upper half of normal range.
One study showed lower IQ in infants with T4 concentration below 10 μgm/dl during first year of life along with TSH above 15 μU/dl compared with those having T4 concentrations more than 10 μgm/dl. Higher doses of Levothyroxine (l-thyroxine) have been associated with better intellectual outcome in children with CH. However, some studies have shown that higher doses of Levothyroxine may result in behavior problems like increased anxiety, social withdrawal and poor concentration at age of 8 years demonstrating thus potential dangers of overtreatment with levothyroxine in CH children.
Congenital hypothyroidism (CH) is one of the most common preventable cause of mental retardation. The best way to detect infants with CH is by screening large populations of newborns. If the diagnosis is made and treatment started within a few weeks of birth, neurodevelopmental outcome generally is normal. The etiology of the most common cause of CH, thyroid dysgenesis, is largely unknown as the increase incidence of CH.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Giselle Pentón-Rol.
