AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2641-0419/139Copyright
1Bundeswehrzentralkrankenhaus Koblenz, Klinik I, Rübenacher Str. 170, 56072 Koblenz, Germany 2Medizinische Klinik und Poliklinik II, Universitätsklinikum Bonn, Venusberg-Campus 1, 53127 Bonn, Germany 3GFO Kliniken Bonn, Robert-Koch-Str. 1, 53115 Bonn, Germany
*Corresponding Author: Debabrata Dash, Department of Cardiology, Zulekha Hospital, Sharjah, UAE
Citation: Debabrata Dash, Sreenivas Reddy, Rohit Mody, Shahid A Merchant., (2021) Managing Calcified Coronaries: the Bugaboo of Percutaneous Coronary Intervention. J. Clinical Cardiology and Cardiovascular Interventions, 4(5); Doi:10.31579/2641-0419/139
Copyright: © 2021 Debabrata Dash, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 February 2021 | Accepted: 19 March 2021 | Published: 26 March 2021
Keywords: percutaneous coronary intervention; atherectomy; lithotripsy
Background
Percutaneous coronary intervention (PCI) of lesions with heavily coronary artery calcium (CAC) still represents a challenge for interventionists, with increased risk of immediate complications, late failure due to stent underexpansion and malapposition, and consequently poor clinical outcome. In this focused review, we provide the summary of principles, technique and contemporary evidence for various existing and emergent plaque modifying strategies.
Main text
PCI of lesions with heavy CAC still poses a challenge for the interventionists due to an increased risk of incomplete lesion preparation with subsequent suboptimal stent deployment and higher rates of acute and chronic stent failure. With the emergence of many novel devices and technologies, the treatment of lesions with heavy CAC has become increasingly feasible, safe and predictable. It seems likely that combining enhanced intravascular imaging modalities with traditional or new dedicated tools for the treatment of such lesions grant better lesion preparation. This optimizes delivery and deployment of drug-eluting stents translating into improved patient outcome.
Conclusion
The lesions with significant CAC are likely to surge due to aging population and increased rates of diabetes and chronic renal disease. The optimal therapy for such lesions is multi-adjunctive and requires the availability of several modalities including intracoronary imaging which could impact the clinical outcome favourably.
Heavy coronary artery calcium (CAC) poses a real challenge for successful percutaneous coronary intervention (PCI). Treatment of such calcified lesions lead to higher rates of procedural complications, [1] with higher rates of target lesion revascularization (TLR), restenosis, and major adverse cardiac events (MACE). [2-5] Heavily calcified lesions are prone to stent underexpansion and malapposition, which are associated with higher rates of stent thrombosis as well as in-stent restenosis. [6-7] Several strategies and technologies have been crafted to treat CAC with the aim of optimal lesion preparation followed by successful stent deployment. Advances include balloon-based (cutting and scoring balloon, super high pressure balloon and lithoplasty balloon etc) and atherectomy (rotational, laser, and orbital) techniques. Here, the author describes the utility of such modalities in contemporary practice.
2.1 Pathophysiology of CAC
CAC is an active process reflecting a wider systemic inflammatory status, typically observed in patients with metabolic syndrome, diabetes mellitus, or chronic kidney disease. [8,9]It is more common in men older than 70 years of age (>90% in men vs. 67% in women). [10]The incidence of CAC varies according to the imaging modality used. The moderate to severe CAC can be encountered in up to one-third of coronary lesions in coronary angiography (CAG). [11] Atherosclerotic CAC is dysmorphic calcium precipitation created by chondrocyte-like cells and linked to expression of inflammatory factors, such as cytokines released by tissue macrophages and foam cells. It is likely that inflammation precedes calcification and plays an important role in its progression, with the two processes coexisting and promoting each other. [12]CAC is commonly associated with larger plaque burden, multivessel disease and a greater degree of lesion complexity including involvement of coronary bifurcation or chronic total occlusion.11Moreover, specific patterns of CAC, such as calcified nodules and coronary microcalcifications, are related to plaque instability and vulnerability. [13] Typically, these lesions are challenging to cross with standard devices and are less likely to respond to conventional balloon dilatation. Inevitably, inadequate lesion preparation before stenting increases the risk of stent loss, stent underexpansion/fracture and the rate of intraprocedural complications, such as no reflow, coronary dissection, or perforation. [11]Interestingly, the passage of drug-eluting stents (DES) through areas of heavy CAC has also been related to polymer damage with consequent impairment of drug elution.
2.2. Imaging techniques
2.2.1 Coronary computed tomography angiography
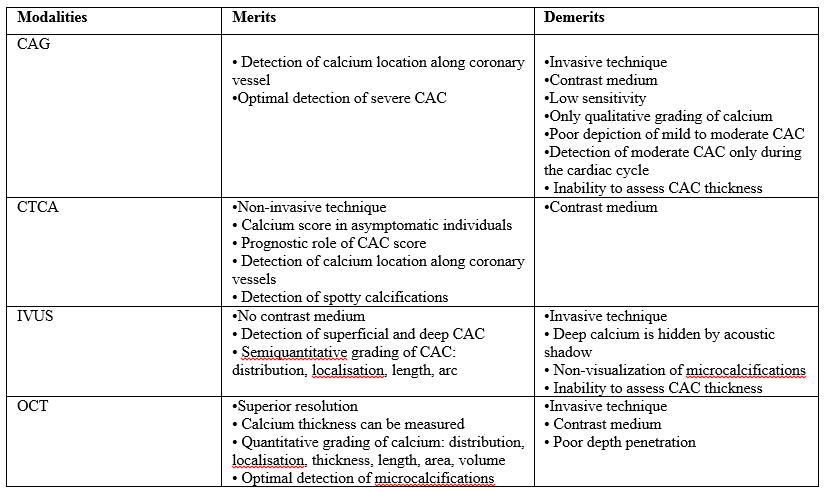
Coronary computed tomography angiography (CCTA) is the most important non-invasive imaging technique used. CAC is depicted as an area of hyperattenuation, defined as an area of at least 1 mm2 with >130 Hounsfield units or ≥3 adjacent pixels using the Agatston method. [14] A CAC score is calculated using a weighted value assigned to the highest density of calcification in each coronary segment that is multiplied by the area and summed finally for all arteries to give a total coronary calcium score correlated with the patient outcomes. [15] This score carries a strong prognostic factor for clinical events in the mid to long term in asymptomatic population. CCTA may uncover spotty calcification which is designated one of the signs of plaque vulnerability. This modality allows accurate identification and localization of calcium along coronary arteries thereby improving procedural success of PCI.
2.2.2 Coronary angiography
Coronary angiography (CAG) is often limited by underestimation of calcium, inaccurate grading, and inability to assess calcium depth within the plaque. CAC is classified as none or mild, moderate, or severe. The radiopacity observed only during the cardiac cycle before injection of contrast medium defines moderate CAC. Severe CAC is delineated as radiopacity observed without cardiac motion, visible on both sides of the arterial lumen, as a double track. [11] The calcium content tends to appear as hazy areas with inhomogeneous contrast staining and hence the differentiation from thrombus is difficult using CAG only. CAG is able to determine CAC only in 38% of cases and the identification seems to be dependent on the degree of the arch of calcification (60% for moderate and 85% for severe CAC) as demonstrated by Mintz et. [16]
2.2.3 Intravscular ultrasound
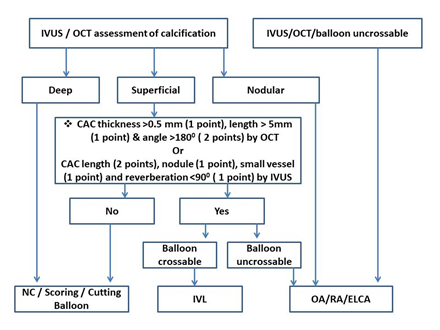
The hallmark of CAC on intravascular ultrasound (IVUS) is an echodense plaque that is brighter than reference adventitia with acoustic shadowing. One of the limitations of IVUS is that dense fibrous tissue may also cast a shadow similar to CAC. CAC brings about reverberations in contrast to dense fibrous tissue. IVUS enhances the sensitivity to in detect CAC significantly compared with CAG (73% of cases vs. 38%; p < 0.001). [16] Quantitatively (the arc of lesion), CAC has been classified into 4 classes on IVUS: Class I, 0°–90° calcification; Class II, 91°–180° calcification; Class III, 181°–270° calcification; and Class IV > 270° calcification. [17] Semiquantitative grading classifies CAC as absent or subtending 1, 2, 3, or 4 quadrants. IVUS determines abluminal calcified deposits within the deeper layers (media or adventitia) of the vessel wall. It allows only definition of the calcific arch, without offering insights into accurate thickness of CAC because of acoustic shadowing. Maximum circumferential extension of calcium >180° is linked to possible stent underexpansion. An IVUS CAC score (Figure 1) of ≥ 2 (2 points for calcium length >2700 > 5 mm, 1 point each for calcium nodule, smaller vessel diameter (<3.5 mm) and reverberation <900) emerges as a relevant predictor for stent underexpansion warranting adjunctive device. [18]

2.2.4 Optical coherence tomography
CAC is designated as signal-poor or heterogeneous region with sharp delineated borders in Optical coherence tomography (OCT). Unlike IVUS, where CAC is most often confused with dense fibrous tissue, OCT detected CAC very often simulates lipid or necrotic core; however, the signal-poor regions of CAC are sharply delineated whereas the signal-poor regions of lipid or a necrotic core have poorly defined or diffuse borders. [19] OCT can measure CAC thickness better due to higher resolution, but may miss deep calcifications because of insufficient penetration. OCT can measure CAC thickness, area, and volume, and automatic quantification of these parameters may be possible (Table 1). [20] A lesion with CAC score of 4 (2 points for CAC angle >1800, 1 point for CAC thickness >0.5 mm, and 1 point for CAC length >5 mm) in OCT has emerged as a reliable predictor for stent underexpansion (stent expansion <70%) as proposed by Fujino et al. [21]
2.3. Treatment modalities
A key concept in approaching heavily CAC involves facilitation of lesion crossing and plaque modification. The support wires, buddy wires, guide extensions, lesion predilatation and anchoring of the guide catheter with inflation of a second balloon in a side branch or distal vessel are possible means for lesion crossing. The underlying calcified plaque gets modified using the dedicated balloon-based (Table 2) and/or ablation (Table 3) devices.

2.3.1 Balloon-based strategies
2.3.1.1 High and super high pressure non-complaint balloons
A non-complaint (NC) balloon may be the first choice in mild to moderate calcified stenosis with restricted calcium arc (<90°). However, the risk of eccentric balloon expansion because of the increased hoop stress conferred by severe CAC, is not fully mitigated by NC balloon. The focal points of resistance within a lesion result in nonuniform balloon expansion and "dog boning" with hyperexpansion in the more compliant segments of the vessel without fracturing the calcium.
Super high-pressure balloon technology incorporates a rapid-exchange NC balloon (OPN Sys Medical, Frauenfeld, Switzerland) with a twin-layer structure allowing inflation pressure up to 35 to 40 atm without bursting of the balloon (Table 2). This is considered as not only effective but also safe approach when experiencing extremely calcified lesions undilatable by conventional high-pressure NC balloon. Although this balloon can be used both before and after stent implantation, most evidence confirms safety and efficacy during post stenting dilation. The unique twin-layer technology ensures uniform balloon expansion over a wide range of pressures, reducing the risk of balloon rupture, vessel damage and coronary perforation. [21] The main limitation of the OPN NC balloon is its relatively high profile which, together with the stiffness of the twin-layer technology, undermines any attempt to recross when inflated. Guide extension catheter may assist successful delivery of such balloon. [22]
2.3.1.2 Cutting and scoring Balloons
The cutting balloon ([FlextomeTM], Boston Scientific, Natick, MA, USA) is a semi-compliant monorail over-the-wire (OTW) balloon with 3 or 4 microtomes mounted on its body, designed to cut the continuity of fibrocalcific plaque creating fissures on the plaque. The cutting balloon ensures a more controlled lesion predilation with less adjacent vessel wall trauma and less risk of dissection. The presence of cutting elements on the surface of the balloon allows effective dilation with a lower inflation pressure (Figure 2).

The microblades also prevent the balloon slippage is prevented by the microblades. One randomized trial failed to show a superiority of cutting balloon for type A/B lesions compared with standard balloons. [23] An IVUS-based study [24] indicated that cutting balloon achieves larger luminal gain compared to conventional balloon. It is limited by high rigidity that hinders lesion navigation through tortuous and calcified vessels. With its most recent iteration (Wolverine) the atherotome’s support thickness has been reduced, without affecting the functional height of the blade, resulting in an overall smaller crossing profile and improved crossability.
The principle of using a “buddy wire” to fracture calcified plaque promoted the development of the scoring balloon: a low-profile semicompliant balloons with a scoring element on the surface (AngioSculpt, Biotronik, Berlin Germany; Scoreflex OrbusNeich, Hong Kong, China; NSA Alpha BBraun, Melsungen, Germany). [25] During inflation, the radial force is mainly exerted on the scoring element and this is transmitted to the vessel wall causing plaque fissuration (Table 2). The embedded nitinol element ensures anchoring of the balloon with a lower risk of “melon-seeding” effects and a lower risk of dissection and perforation. It is likely that prolonged inflation might improve the device navigation with a “creep phenomenon”: a sustained tensile load ensuring microcrack formation and propagation leading to a phasic tissue elongation. [26] Scoring balloons have been considered as an alternative to cutting balloons in moderate calcification and, in recent years, have been preferred due to superior flexibility and deliverability, although no specific randomised control trials exist in the literature so far.
2.3.1.3 Constrained semi-compliant balloon (chocolate balloon)
The chocolateR balloon (TrirReme Medical, Pleasanton, CA, USA) is an OTW balloon with a mounted nitinol constraining structure specifically designed for uniform, controlled inflation and a rapid deflation ensuring an atraumatic dilatation obviating the need for cutting or scoring balloons (Table 2). The nitinol constraining structure generates balloon segments or "pillows" that make contact with the vessel and functions to minimize local forces. The "grooves" promote plaque modification. The distinctive pillows and grooves minimize vessel trauma, reduce the rate of dissection. [22]
2.3.1.4 Intravascular lithotripsy
Intravascular lithotripsy (IVL) is the most recent armamentarium for the treatment of lesions with heavy CAC. It delivers localized pulsatile sonic pressure waves, modifying preferentially calcific plaque without affecting the soft tissue, and subsequently promoting stent delivery and optimization. [27] The balloon catheter with multiple lithotripsy emitters is negotiated over a guidewire to the target lesion. The balloon is attached to the external pulse generator. With balloon inflation at low pressure (4 atm), a burst of 10 pulses of high energy is delivered over 10 seconds followed by further balloon inflation at 6 atm for 15-20 seconds before deflation. This process can be repeated to a total of 8 cycles per balloon (80 pulses). The balloon sizing is based on the desired stent size for that target lesion (ie, 1:1 for the reference vessel diameter) and is often guided by intracoronary imaging. [28] The IVL balloons are all 12 mm long with diameters ranging from 2.5 mm to 4.0 mm. Guide catheter extenders and buddy wire support may be required for deliverability and positioning of this large profile balloon.
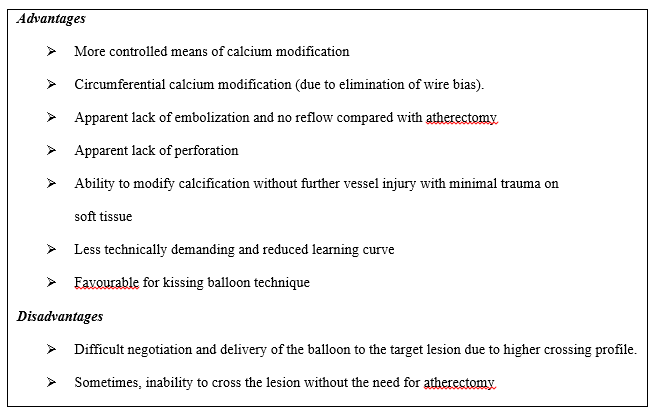
By inducing calcium fractures (as assessed with IVUS or OCT)., [29-31] the IVL therapy achieves optimal stent expansion in undilatable specialty balloons and rotational atherectomy (RA) refractory lesions. The navigation of IVL balloon could be impacted by severe tortuosity or angulation, critical lumen reduction, plaque indentation into the lumen and a small vessels and multiple stent layers. Up to 46% of the lesions might also require dedicated lesion predilatation and/or post-dilatation with NC balloons or could benefit from other adjunctive devices such as cutting or scoring balloons or atherectomy to either facilitate balloon delivery or increase calcium compliance after IVL therapy. [30,32] IVL targets CAC circumferentially and thus avoids guidewire bias. Reduced learning curve, apparent lack of embolization and perforation are all very attractive attributes of IVL as compared to atherectomy (Table 3). [22] Furthermore, IVL is possible following stenting. Unlike RA, IVL can be used with more than one guidewire to protect side branches. Because of the presumed ability to pass across a second balloon, IVL can be used with the kissing balloon technique.
This modality can cause vessel complications although balloon rupture is uncommon. The sudden balloon burst has been described with arterial dissection during lithotripsy therapy. Recently there is a case report of perforation following this therapy.33 Furthermore, vessels with a diameter >4 mm (maximum shockwave balloon size) or important plaque eccentricity preclude appropriate IVL balloon apposition to the vessel wall, and may reduce the efficacy of the therapy. IVL could be safely performed with high procedural success, minimal complications with substantial calcific plaque fracture in most lesions in a prospective multicenter Disrupt CAD II study. [34]
2.3.2 Atherectomy or ablative devices
A strategy of debulking calcified lesions as a part of bail-out technique to address heavy CAC has evolved into a primary lesion preparation approach called primary atherectomy in contemporary practice. Compared to bail-out strategy, the primary atherectomy is associated with decreased procedural and fluoroscopy times, contrast volume, and the number of predilatation balloon catheters used. [35] This alters plaque morphology, inflicting fractures in heavy CAC and changing lesion compliance, to increase the likelihood of maximal MLD and complete stent expansion.
2.3.2.1 Rotational atherectomy
Rotational atherectomy (RA [Boston Scientific, Marlborough, Massachusetts]) system is composed of a high-speed rotating diamond-coated burr aimed to act as an abrasive rotatory surface against calcific plaque. The elliptic-shaped metallic burr is available in different sizes (from 1.25 to 2.5 mm) and is mounted over an advancer (RotaLink) drive-shaft connected to a motor that converts compressed gas into rotational energy. The burr is advanced over a Rotawire (dedicated 0.009-inch 325 cm long wire) designed to maximize flexibility and to minimize wire bias. The recently introduced RotaPro (Boston Scientific) represents an updated iteration and it offers a better user interface and controls integrated on the advancer. Applying the principle of "differential cutting" RA acts preferentially the fibrocalcific plaque tissue while sparing elastic tissue (Figure 3).
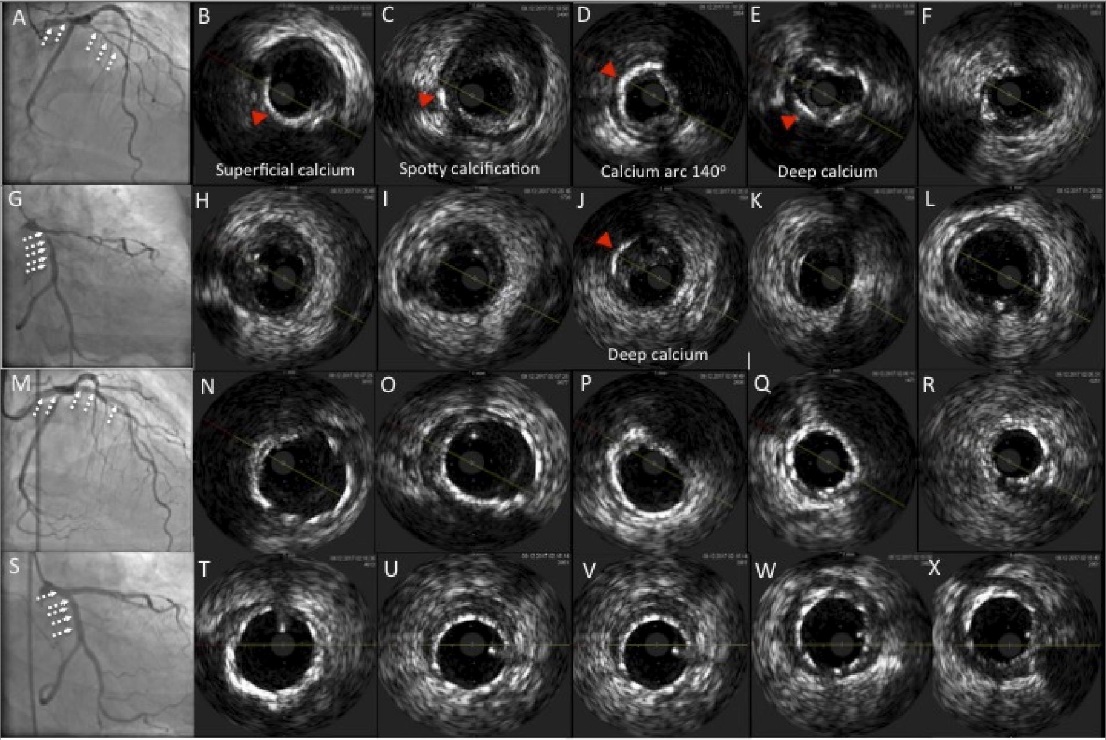
A-F: Baseline lesion in left anterior descending (LAD)
G-L: Baseline lesion in left circumflex (LCX)
M-R: Final result after RA followed by left main bifurcation stenting
S-X: Final result after RA followed by left main bifurcation stenting
A, G, M, S: Angiographic images
B-f, H-L, N-R, T-X: IVUS imaging
Figure 3. Intravascular ultrasound (IVUS) depiction of the effects of rotational atherectomy (RA) on heavy coronary calcium
The ablated tissue is pulverized in 5 to 10 mm debris, which are released into the distal coronary microcirculation. This is the likely mechanism underlying the potential for transient slow/no reflow following RA. [36] The wiring technique has been facilitated by the use of a regular workhorse wire or hydrophilic wire subsequently exchanged over microcatheters or OTW balloons with the rotawire. The RA results are affected by CAC eccentricity, vessel luminal area, burr size and wire bias degree. [37] An optimal scenario for RA in terms of predictable luminal gain is a lesion with concentric circumferential calcium (cross-section >2700 of CAC) and a minimal lumen area smaller than the burr size. Complications of RA include burr entrapment, coronary dissection, and perforation but their occurrence can be usually minimized by optimal technique. Fundamental elements of contemporary optimal technique include use of a single burr (1.5 mm) with burr-to-artery ratio of 0.6, rotational speed of about 140,000 to 180,000 rpm, gradual burr advancement using a pecking motion, short ablative runs (15 to 20 s), and avoidance of decelerations >5000 rpm. However, in lesions not crossable with a 1.5-mm burr or in very long tortuous segments; a 1.25-mm burr with stepwise escalation may be necessary. [38]
ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) [39] trial failed to demonstrate a superiority of RA versus conventional balloon dilatation before DES implantation in heavy CAC. Upfront high-speed RA is feasible in nearly all patients and improves the success of DES deployment compared with modified cutting or scoring balloons, according to results of the contemporary Comparison of Strategies to PREPARE Severely CALCIFIED Coronary Lesions (PREPARE-CALC) trial. Although both strategies ensure equal safety and efficacy, the use of RA is no longer associated with excessive late lumen loss in the modern era. [40]
2.3.2.2 Orbital atherectomy
Orbital atherectomy (OA) is another novel treatment modality for heavy CAC. [31] It consists of an eccentrically mounted diamond-coated 1.25-mm crown, connected to a drive shaft and to a controller powered by a pneumatic console (CSI Diamond 3600 Coronary Orbital Atherectomy System, St. Paul, Minnesota). Compared with the rotaburr, which only allows calcium ablation during forward advancement, the crown of OA with diamond chips both on front and back, enables bidirectional atheroablation (Table 4).
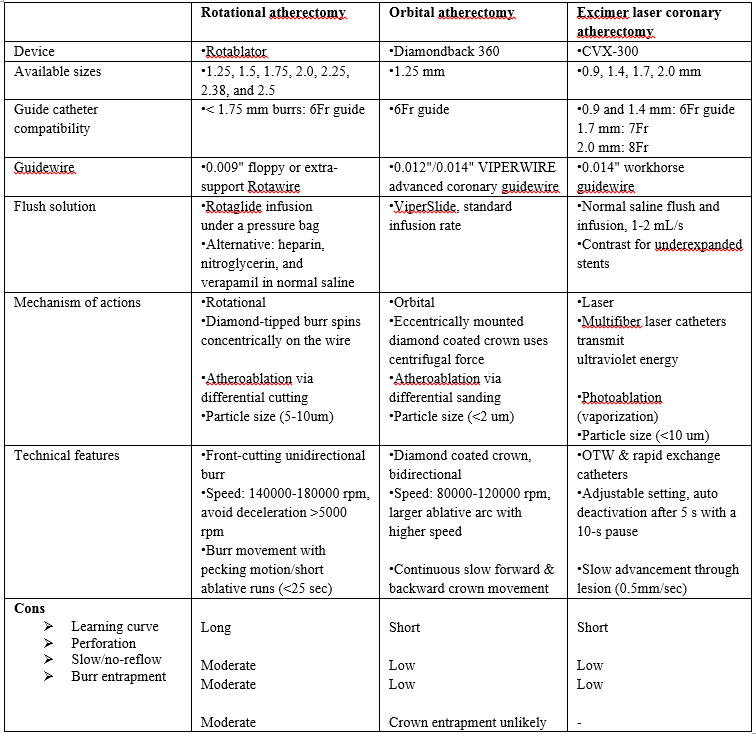
The crown entrapment is less likely as compared to burr entrapment due to retrograde ablation. The crown is advanced over a dedicated (ViperWire Advance, St. Paul, Minnesota) a 0.014-inchwire, with superior maneuverability compared with the 0.009-inch Rotawire. Using the controller, the operator can move the crown forward and backward and can regulate the speed of the crown orbit (80,000 to 120,000 rpm). OA incorporates centrifugal forces which pushes and compresses the crown against the plaque with a “sanding” action of the calcified component. OA might have a selective action on the rigid calcified component, whereas healthy elastic tissue may be spared. Whereas the RA burr is moved forward in a slow, pecking motion to allow intermittent ablation; the OA crown is advanced with a gradual, continuous motion, even interrupting in a region of interest to permit more time for ablation. Notably, by increasing its orbit as rotational speed increases, OA allows ablation of CAC using the same device (1.25-mm crown) in vessels up to 3.5-mm diameter. Other advantages of OA include the 6-F guiding catheter compatibility, smaller size of particles released during ablation (2 vs. 5 to 10 mm in RA), no interruption in blood flow during crown orbiting, and less vascular heating.
For moderate degree of CAC, the lesion preparation could be achieved with balloon-based approaches. Conversely, higher degree of CAC may require more aggressive ablative approaches, such as ELCA, RA or OA. Because of its ease of use, shorter
learning curve, and unique action on both superficial and deep CAC, IVL has the potential of more widespread adoption.
The authors feel that there would be a surge in a hybrid approach involving drill (RA or OA) and shock (IVL) in near future. Despite the growingdata for various modalities, additional randomized controlled trials are warranted to further clarify the superiority of one modality over another.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Matteo Bonori.

I recommend without hesitation submitting relevant papers on medical decision making to the International Journal of Clinical Case Reports and Reviews. I am very grateful to the editorial staff. Maria Emerson was a pleasure to communicate with. The time from submission to publication was an extremely short 3 weeks. The editorial staff submitted the paper to three reviewers. Two of the reviewers commented positively on the value of publishing the paper. The editorial staff quickly recognized the third reviewer’s comments as an unjust attempt to reject the paper. I revised the paper as recommended by the first two reviewers.

Dear Maria Emerson, Editorial Coordinator, Journal of Clinical Research and Reports. Thank you for publishing our case report: "Clinical Case of Effective Fetal Stem Cells Treatment in a Patient with Autism Spectrum Disorder" within the "Journal of Clinical Research and Reports" being submitted by the team of EmCell doctors from Kyiv, Ukraine. We much appreciate a professional and transparent peer-review process from Auctores. All research Doctors are so grateful to your Editorial Office and Auctores Publishing support! I amiably wish our article publication maintained a top quality of your International Scientific Journal. My best wishes for a prosperity of the Journal of Clinical Research and Reports. Hope our scientific relationship and cooperation will remain long lasting. Thank you very much indeed. Kind regards, Dr. Andriy Sinelnyk Cell Therapy Center EmCell

Dear Editorial Team, Clinical Cardiology and Cardiovascular Interventions. It was truly a rewarding experience to work with the journal “Clinical Cardiology and Cardiovascular Interventions”. The peer review process was insightful and encouraging, helping us refine our work to a higher standard. The editorial office offered exceptional support with prompt and thoughtful communication. I highly value the journal’s role in promoting scientific advancement and am honored to be part of it. Best regards, Meng-Jou Lee, MD, Department of Anesthesiology, National Taiwan University Hospital.
