AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1045/103
1 Endocrine oncology. National Cancer Institute. Bogotá DC, Colombia.
2 Endocrinology, Hospital de San Jose. Bogotá DC, Colombia.
3 Radiologist. National Cancer Institute. Bogotá DC, Colombia.
*Corresponding Author: Andrés Flórez R, Endocrinology, Hospital de San Jose. Bogotá DC, Colombia.
Citation: Luis F. F-Maya, A Flórez R, Angélica M. G-Clavijo, A A. Cuellar C, M Tapiero G, et al. (2021) Management of Advanced Medullary Thyroid Carcinoma with Vandetanib: Case Series J. Endo and Dis; 5(1); DOI:10.31579/2640-1045/103
Copyright: © 2021, Andrés Flórez R, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 February 2021 | Accepted: 11 March 2021 | Published: 15 March 2021
Keywords: medullary thyroid cancer; vandetanib; tyrosine kinase inhibitors; safety; retmutation
Objective: To describe the tumor response and adverse events in patients with advanced medullary thyroid carcinoma (MTC) treated with vandetanib at the National Cancer Institute in Bogotá, Colombia.
Materials and Methods: Case series including five patients with advanced MTC treated with vandetanib from April 2011 to August 2018 and a minimum follow-up of 6 months.
Results: 5 patients met the inclusion criteria, including 3 women. The mean age was 49 years. A total of 4 patients underwent total thyroidectomy prior to starting vandetanib. The main indication for vandetanib was progression of liver metastasis (4 patients). Regarding treatment response, 3 patients presented stable disease, 1 patient showed partial response, and 1 had disease progression. The mean treatment duration was 16.5 months. Grade 3 or 4 adverse events were observed in three patients, 1 with diarrhea, 1 with hypertension, and 1 with rash. All symptoms improved with dose reduction or temporary suspension of vandetanib.
Conclusions: The management of advanced MTC with vandetanib allows for prolonged disease control (stable disease or partial response). Although adverse events are frequent, most are mild and severe cases are manageable.
Medullary thyroid carcinoma (MTC) accounts for 1–2% of all types of thyroid cancer in the United States [1]. The disease can occur sporadically (75%) or be inherited (25%) [2] Germline mutations of the RET oncogene are identified in multiple endocrine neoplasia (MEN) 2A or 2B and familial MTC [3] and are characterized by different clinical presentations according to the variant type. Somatic mutations of this gene are found in 50% of sporadic MTCs [4]. RAS gene mutations have been described in 68–81% of the patients with MTC without mutations [5,6].
The treatment of choice for MTC is total thyroidectomy with central neck dissection and, depending on the case, lateral neck dissection [1]. Patients with MTC commonly present with extensive regional involvement or distant metastatic disease at diagnosis or during follow-up, which hinders achievement of cure with the initial surgical intervention [2]. The overall survival at 10 years in patients with metastatic disease is 40% [7]. The therapeutic options in cases of advanced MTC include palliative surgery, radiotherapy, locoregional therapies, and systemic treatment with tyrosine kinase inhibitors (TKIs) such as vandetanib [1].
In the current research, we present 5 patients with advanced MTC who required therapy with vandetanib and progressed with disease control (stable disease and partial response). We also report the adverse events (AEs) observed with therapy.
The study included patients with a diagnosis of MTC confirmed by the pathology service at the National Cancer Institute, with either hereditary or sporadic disease. Presence of advanced disease defined by the occurrence of distant metastases with progression in the previous year according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 [8], who were managed with vandetanib and had a minimum follow-up period of 6 months after treatment start. A search of medical records was conducted between April 2011 (when the Food and Drug Administration [FDA] approved vandetanib) and August 2018.
Diagnostic images were obtained 0–3 months before the start of vandetanib (pre-TKI) and every 3 months thereafter. The imaging tests included non-contrast chest computed tomography (CT), abdominal CT with contrast, or magnetic resonance imaging (MRI) with arterial-phase contrast enhancement, and additional studies according to specific involvement (e.g. spinal MRI). A single INC radiologist (CCC) reviewed the images to decrease interobserver variation. Tumor response was evaluated according to RECIST version 1.1 [8], disease control rate (DCR) was defined as the proportion of patients who show, complete response, partial response (PR) or stable disease (SD). Progression rate was considered as the time in weeks elapsed between the last diagnostic image showing stable disease and the image showing progression (pre-TKI). The time (in weeks) elapsed between the diagnosis of progression and the start of treatment was recorded.
Clinical and laboratory follow-up was carried out in the following time points: before treatment start, week 2, month 1 and 3, and every 3 months thereafter. Clinical follow-up was carried out by the coauthors of this paper. Treatment-related adverse events (AEs) assessed with the Common Terminology Criteria for Adverse Events (CTCAE ) version 5.0 [9], body weight, blood pressure, and findings from physical examination were recorded at each assessment. Body weight was measured with a Health o Meter professional scale® (Sunbeam Products, Boca Raton, Florida, USA) and recorded in kilograms (kg). Blood pressure was measured with a blood pressure monitor (Vismo, Nihon Kohden, Tokyo, Japan) and recorded in mmHg. Clinical laboratory tests and diagnostic images were performed at the INC. Laboratory tests requested prior to treatment start included TSH, creatinine, transaminases (AST and ALT), complete blood count (CBC), hepatitis B surface antigen, hepatitis C antibodies, calcium (Ca), potassium (K), magnesium (Mg), and electrocardiogram (ECG). Complementary tests requested during follow-up included TSH, CBC, creatinine, AST, ALT, Ca, K, Mg, and ECG. Bazett’s formula [10] was used to calculate the corrected QT interval (QTc), and the result was recorded in milliseconds (ms). All patients underwent a RET mutation analysis, and the presence or absence of the mutation and the type of mutation were documented.
Of 10 patients identified, 5 were excluded due to a follow-up period shorter than the predetermined one or due to incomplete data for analysis. Of the 5 patients included, 3 were women. The mean age at diagnosis was 37 years. Only one case of germline RET mutation was identified in a patient with a diagnosis of pheochromocytoma and lichen cutaneous amyloidosis (Patient 4: c634r mutation). The characteristics of the patients in terms of staging, metastatic site, and relapse are described in Table 1. Prior to initiating the TKI, Patients 4 and 5 had chronic diarrhea, which was attributed to elevated serum calcitonin; however, the diarrhea failed to improve after treatment start, despite the reduction in calcitonin levels.
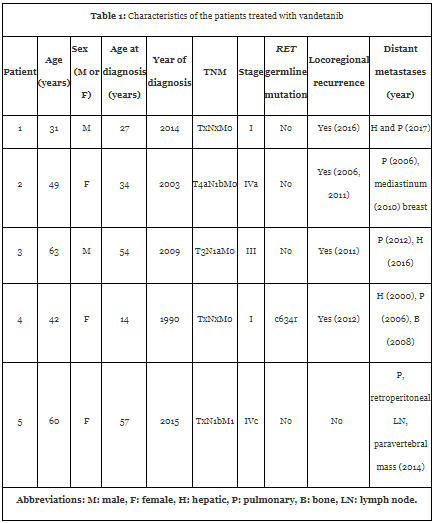
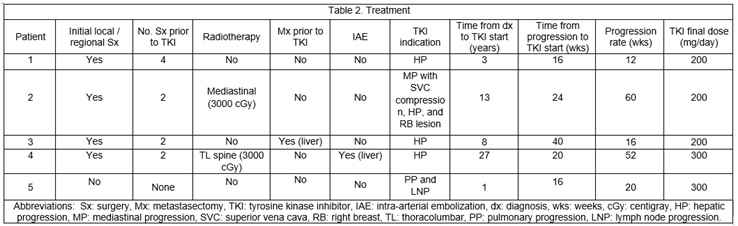
Table 2 presents the types of treatment received by the patients before the start of TKI and the indications for initiation of therapy. Vandetanib was started between 1 and 27 years after the diagnosis. Patient 4, who had the longest disease duration, received sorafenib for 8 months, 2 years before starting vandetanib, until progression was demonstrated. In all patients, the starting dose of vandetanib was 300 mg/day; however, due to side effects, the dose was reduced to 200 mg/day in 3 of 5 patients. The biochemical response (levels of calcitonin and carcinoembryonic antigen) was irregular and showed no correlation with the structural response.
The mean treatment duration with vandetanib was 16.5 months (6 to 27 months). Patient 2 had the longest follow-up (27 months) and presented stable disease at the time of data collection for the present study, although it should be noted that the size of the lesions increased by 14% at month 24 compared with baseline. A total of 3 patients presented stable disease, 1 patient had partial response, and 1 had progression of liver lesions 12 months after beginning treatment. Table 3 shows the tumor response by patient. Figure 1 shows the abdominal MRI of Patient 1, showing stable response at month 12 at the hepatic level. Figure 2 shows partial response at month 24 in Patient 5.



The most frequent AEs, mean time for emergence of AEs after TKI start, and mean duration of symptoms are shown in Table 4. Most AEs were grade 1 or 2. The most frequent AEs observed in the first 8 weeks post-TKI were diarrhea (2 patients), creatinine elevation (2 patients), and TSH elevation (4 patients). The most frequent dermatological symptoms were acne (patient 1), hand-and-foot syndrome and rash (patient 2), and photosensitivity (patients 3 and 4). Figure 3 shows the photosensitivity reaction presented by patient 3. The patients with dermatological AEs received topical management recommended by a dermatologist. Grade 3 or 4 AEs included diarrhea (1 patient), hypertension (1 patient), and rash (1 patient). Patient 3 presented grade 3 diarrhea (10 to 15 episodes daily), which started 4 weeks post-TKI and resolved after a decrease in vandetanib dose. Patient 2 presented grade 3 hypertension at 2 weeks post-TKI, which was controlled with antihypertensive drugs and a reduction in TKI dose.


Advanced MTC comprises locally aggressive disease that is not susceptible to surgical resection along with metastatic disease [2,11]. Locoregional involvement is associated with a decrease in 5-year recurrence-free survival, rates of 75% with localized thyroid disease versus 66% with regional involvement [12] and decreased overall survival with an increase in the number of lymph nodes involved; the rates of overall survival according to the number of lymph nodes involved (in parentheses) are 76% (1–5), 74% (6–10), 61% (11–15), and 69% (≥ 16) [13]. All our patients had regional lymph node involvement, which was evident at diagnosis in three patients.
Metastatic disease can be detected at diagnosis in 4–17% of the patients and during follow-up in 18–38% of them. The metastases usually affect the liver (67–69%), lung (54–60%), and bone (34–51.1%) and less frequently the brain, breast, and soft tissues [2]. The most frequent metastatic sites in our patients were the lungs in 5 patients and liver in 4 patients, and in all except one patient (patient 5), the metastases were detected during follow-up. In contrast to higher rates of bone metastases described in the literature, only one patient in our study presented bone involvement. One patient had metastases to the breast, which are rare, as mentioned above. Metastatic disease can be asymptomatic or may present with symptoms related to local involvement or increased hormonal production (diarrhea, flushing, and less frequently, ACTH-dependent Cushing’s syndrome) [2]. Two patients in this case series presented calcitonin-associated diarrhea and did not respond to management with TKI.
The objectives of treatment in locally aggressive MTC are pain control, prevention of upper airway involvement, maintenance of phonation and swallowing, and preservation of parathyroid function and shoulder mobility [1]. In these cases, the decision to perform a surgical procedure must be based on the impact of the disease on vital structures (airway and/or digestive tract), with the objective of preserving the functionality of these organs and reducing complications [1,14]. This was the case in Patient 1, who had a mediastinal mass resected due to compression of cranial nerves IX and X, and in Patient 2, in whom there was a risk of vascular compression.
Pulmonary metastases are often micronodular and multiple [1,2]. None of our patients received local therapy due to metastatic pulmonary involvement. Hepatic metastases are generally multiple; thus, surgery is not feasible in most cases. In Patient 3, metastasectomy was performed taking into account a very localized metastatic disease, but the patient developed progression 1 year after the procedure. Local therapies such as ablation, transarterial embolization or chemoembolization, may be useful in selected cases [1], as in Patient 4, who underwent intra-arterial embolization to decrease the secretory burden of the tumor and achieved disease control for 4 years. Among bone metastases, the most frequent ones are to the spine (92%), pelvis (69%), and ribs (53%) [15]. Bone metastases may be managed with surgery, radiofrequency ablation, or radiotherapy [2]. Antiresorptive agents, like bisphosphonates or denosumab, improve pain and have an impact on decreasing the emergence of related skeletal events [15]. Radiotherapy of the neck and/or mediastinum allows for local control of the tumor in cases with a high probability of recurrence or when surgical excision cannot be performed or is incomplete, improving relapse-free survival but with no impact on overall survival [1,16]. Patient 2 received mediastinal radiotherapy due to a risk of compression of vital structures 5 years after initial mediastinal resection and had an adequate response for 5 years, when TKI was then recommended.
Systemic therapy such as TKIs or chemotherapy, has a positive impact on progression-free survival (PFS) in patients with MTC and has been associated with partial response or stable disease. This type of therapy should be considered in case of progression and high tumor burden [11,17], but is not recommended in patients with detectable calcitonin without imaging-confirmed metastasis, non-measurable disease (less than 1 cm), or in cases of stable or slow-progressive disease [2,17].
TKIs are used in advanced MTC considering the association of the disease with germline and somatic activating mutations of the RET gene and overexpression of vascular endothelial growth factor receptor (VEGFR) 1-2-3, vascular endothelial growth factor (VEGF)-A, fibroblast growth factor receptor 4 (FGFR-4), platelet-derived growth factor receptor (PDGFR), epidermal growth factor receptor (EGFR), and hepatocyte growth factor (HGF) [18]. While TKIs may decrease calcitonin levels, the decrease not always correlate with a reduction in tumor size. In our patients, the biochemical response was irregular despite an adequate structural response. Currently, the only TKIs that have demonstrated longer PFS and reduction in pain and in symptoms of increased hormonal secretion in randomized, placebo-controlled clinical trials and which are approved by the FDA for treatment of advanced MTC are vandetanib (2011) and cabozantinib (2012) [1]. Vandetanib is a multikinase inhibitor with effects on RET, VEGFR-2, VEGFR-3, and EGFR [18,19]. The effectiveness and safety of vandetanib have been demonstrated in two phase 2 studies of hereditary MTC [20,21]. Robinson et al. [20] reported partial response in 16% and stable disease in 53% of their patients for 24 weeks using a vandetanib dose of 100 mg/day. Wells et al. [21], using a vandetanib dose of 300 mg/day in 30 patients with advanced MTC, reported partial response (PR) in 20% and stable disease (SD) in 53% of the cases, with a median PFS of 27.9 months (95% confidence interval [CI] 19.4-not reached). The ZETA study [22] was a phase 3, multicenter, randomized, double-blind, placebo-controlled, cross-over trial of vandetanib 300 mg/day in 331 patients with hereditary and sporadic advanced MTC with stable or progressive disease. The PFS was statistically significant (hazard ratio [HR] 0.46; 95% CI 0.31–0.69; p < 0>
The indication for vandetanib treatment in our patients was disease progression, and the medication obtained DCR in 4 of our 5 patients, 1 patient with partial response and 3 with stable disease. One patient developed progression after 12 months of stable response. In subgroup analyses, response with vandetanib has been demonstrated regardless of the presence of RET mutation, metastasis location, or baseline tumor burden. A post hoc analysis of the ZETA study in patients with progression and symptoms, 127 patients treated with vandetanib versus 57 treated with placebo, reported a median PFS of 21.43 months (HR 0.43; 95% CI, 0.28-0.64; p < 0>
In the ZETA trial, the most common AEs were diarrhea (56%), rash (45%), nausea (33%), hypertension (32%), headache (26%), and fatigue (24%). A QT interval prolongation of 35 ms compared with baseline was observed in 90% of the participants, while a prolongation of 60 ms was observed in 36% of them [22]. In our study, one of the patients presented grade 1 QT prolongation, with a maximum increase of 44 ms and normalization after reduction of the vandetanib dose to 200 mg/day.
The most common causes of grade 3 or greater toxicity were diarrhea (11%), hypertension (9%), and QT prolongation (8%) [22]. Grade 3 AEs in our series occurred in 3 patients (diarrhea, hypertension, and rash).
While the recommended dose of vandetanib is 300 mg/day, 3 of our patients required a dose reduction to 200 mg/day due to side effects, which did not affect their treatment response. Data are limited in terms of the efficacy of vandetanib 100 mg [20]. A phase 4 study is underway comparing vandetanib 150 mg versus 300 mg in patients with advanced progressive or symptomatic MTC [26].
Cabozantinib inhibits c-MET, VEGFR-2, RET, AXL, FLT-3, and Tie-2, and its effectiveness in MTC was demonstrated in the EXAM study [27], a multicenter, randomized, placebo-controlled phase 3 trial of cabozantinib 140 mg day that included 330 patients with advanced progressive MTC (previous 14 months). The median PFS with cabozantinib was 11.2 months compared with 4 months in the placebo group (HR 0.28; 95% CI 0.19–0.4; p < 0>
The EXAM trial [27] (cabozantinib) included only patients with progressive MTC, as opposed to the ZETA trial (vandetanib), which included patients with progressive and stable disease. This could explain why PFS was greater in the ZETA trial compared with the EXAM trial. None of these studies demonstrated impact of both these TKIs on overall survival; this was possibly related to the slow progression of advanced MTC, which hindered the evaluation of overall survival in the described studies. There are no studies directly comparing cabozantinib with vandetanib, in a real world study of forty-eight patients of which 25 patients received vandetanib as first-line treatment. The PR, SD ≥ 24 weeks and PD in patients taking vandetanib was 26%, 34% and 21% respectively compared to the PR, SD ≥ 24 weeks and PD in patients taking cabozantinib of 22%, 13% and 35% respectively. Median PFS from vandetanib was 17 months and cabozantinib was 4 months. The lower response rates of cabozantinib treated patients is likely due that was mainly used as a second-line treatment after PD on vandetanib. Both TKIs demonstrted similar efficacy in second-line setting (PR around 30% of patients) [28].
Phase 2 studies have found a positive impact of sunitinib 27 and sorafenib 28 in patients with MTC who progressed with vandetanib or cabozantinib, demonstrating rates of partial response of 38% and stable disease of 35% with sunitinib. With sorafenib, rates of partial response have been described at 6.3% and stable disease at 87.5%. Phase 2 studies have also used lenvatinib [29][30] and everolimus [31], but none of these medications has yet been approved for treatment of MTC. Chemotherapeutic agents like dacarbazine, 5-fluorouracil, cisplatin, and doxorubicin, either alone or in combination, have demonstrated partial response or stable disease rates ranging from 10–20%, with a short duration of effect [17,32].
The management of advanced progressive MTC with vandetanib allows for prolonged disease control (stable disease or partial response). While mild AEs are frequent, severe cases resolved without complications after dose adjustment.
ETHICAL APPROVAL
The present investigation was carried out in accordance with the Declaration of Helsinki, national norms set forth in resolution 8430 of October 4, 1993, which classify the study as a “risk-free investigation.” and were in accordance with the ethical standars of the institutional ethics committee. Informed consent was obtained from the patients for registration and publication of pictures and diagnostic images.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest that may affect the impartiality of the reported investigation.
ACKNOWLEDGMENTS
We thank the patients who agreed to participate in the study and who consented to the publication of their pictures and diagnostic images
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
