AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2637-8892/140
1 School of Psychology, Laval University, Quebec, Canada
2 Institute of Nutrition and Functional Foods, Laval University, Quebec, Canada
3 School of Nutrition, Laval University, Quebec, Canada
4 Programme d’Intervention des Troubles des Conduites Alimentaires – Centre Hospitalier Universitaire de Québec, Quebec, Canada
*Corresponding Author: Catherine Bégin, School of Psychology, Laval University, 2325, rue des Bibliothèques, Québec (Québec), Canada, G1V 0A6
Citation: Gagnon C., Grondin S, Côté M., Marie-È. Labonté, Provencher V., Ratté C., Bégin C. (2021) Emotional responses to food pictures according to caloric value in women with an eating disorder. J. Psychology and Mental Health Care. 5(2): DOI: 10.31579/2637-8892/140
Copyright: ©2021 Catherine Bégin, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 August 2021 | Accepted: 01 September 2021 | Published: 08 October 2021
Keywords: affective state; caloric value; eating disorders; emotions; food pictures; nutritional knowledge
Objective: The aim of the current study was to improve the understanding of emotions evoked by food pictures in women with an eating disorder (ED), by distinguishing anorexia nervosa (AN) and bulimia nervosa (BN) diagnoses, while taking into account the caloric content of food and the influence of participants’ nutritional knowledge.
Methods: Thirteen AN, 9 BN and 22 healthy controls (HC) women participated in the study. In a laboratory setting, participants first completed self-report questionnaires regarding their affective state. Then, an emotional rating task of food and non-food pictures was performed in order to examine participants’ emotional reactions to these pictures, depending on the caloric value of the food depicted and controlling for internal state. Finally, an energy density ranking task of food pictures was completed to investigate participants’ nutritional knowledge and its influence on their reactions to food.
Results: Compared to HC, ED participants experienced more fear towards food, which was neither due to their internal state nor to their nutritional knowledge. In AN, fear occurred towards all food, whereas in BN, fear was observed for high-calorie products only.
Conclusion: The key role of food-induced fear in ED was highlighted, particularly in AN.
List of abbreviations
AN: Anorexia nervosa;
BMI: Body mass index;
BN: Bulimia nervosa;
ED: Eating disorders;
HC: Healthy controls;
M: Mean;
SD: Standard deviation.
Introduction
Eating behaviors are known to be influenced by affective states (Aguiar-Bloemer & Diez-Garcia, 2018; Devenport et al., 2019; Macht & Simons, 2000; van Strien et al., 2013). Emotions aroused by food are powerful determinants of individual’s food choices and intakes (Lowe et al., 2016; Martins & Pliner, 2005; Spence et al., 2016). Indeed, positive emotions evoked by food can drive eating behaviors such as disinhibition or craving, whereas negative emotions can lead to its rejection or avoidance (Macht, 2008). This association between food-induced emotions and eating behaviors seems particularly relevant for individuals suffering from an eating disorder (ED) (for review, see Giel et al., 2011). In fact, ED women present altered information processing mechanisms and erroneous thoughts about food and body weight/shape, which modulate negatively their emotional responses towards food and, thus, their caloric intake (Brooks et al., 2011; Coelho et al., 2014; Eiber et al., 2005; Williamson et al., 1999). Due to their enduring nature, these cognitions and reactions contribute to the maintenance and the worsening of patients’ feeding behaviors and their long-term consequences on physical health and psychosocial functioning (Dakanalis et al., 2017; Fairburn et al., 2003; Vitousek & Brown, 2015). Therefore, in order to better understand ED women’s eating behaviors and improve the efficacy of their treatments, it is important to pursue the exploration of emotional responses evoked by food.
In that perspective, Hay and Katsikitis (2014) collected and compared emotional responses generated by food pictures from three groups of women, namely psychiatric controls, ED participants and healthy controls (HC), while adjusting for their initial affective state. This adjustment was important knowing that prevalence of depressive and anxious symptoms is high among individuals suffering from an ED (Aspen et al., 2014; Godart et al., 2015, Morzola et al., 2020 Swinbourne et al., 2012), and considering that such comorbidities can enhance attention allocation to negative stimuli or reduce the experience of positive emotions (Cisler & Koster, 2010; Dai & Feng, 2011; Eizenman et al., 2003; Okon-Singer, 2018). Their results revealed that ED participants gave higher negative ratings (i.e., fear, disgust) and lower positive ratings (i.e., happiness/joy) to food pictures than psychiatric participants and HC. Not only did Hay and Katsikitis (2014) confirm what had already been shown in past studies (e.g., Santel et al., 2006, Rodríguez et al., 2007), but they went further by revealing that the differences between groups remained significant despite the statistical control for women’s pre-experimental affective state, suggesting that negative food-induced reactions could be a core feature of ED. More recently, Foroughi and colleagues (2018) invited HC and women suffering from anorexia nervosa (AN), atypical AN (i.e., with a body mass index [BMI] ≥ 18 kg/m2), bulimia nervosa (BN) and binge eating disorder (BED) to rate their level of happiness, fear and disgust prior to and whilst viewing food pictures. Compared with HC, all groups of ED participants felt more fearful and disgusted when viewing food images, even when their pre-experimental mood was controlled for. However, within the four ED groups, no significant differences were detected, suggesting that aversive responses to food could be a transdiagnosis phenomenon. Although interesting, these results contrast with those of other studies suggesting that individuals with BN behaviors can have positive, or at least, less negative reactions than AN individuals when seeing food (Burmester et al., 2021; Drobes et al., 2001; Friederich et al., 2006; Gagnon et al., 2018; Hoefling et al., 2009; Leehr et al., 2016; Racine et al., 2018).
Furthermore, it has been suggested that emotions induced by food pictures in ED women can differ according to their caloric value. By means of semi-structured interviews inviting participants to freely identify their thoughts (i.e., cognitions, emotions) during the visualisation of food pictures, McNamara and colleagues (2008) showed that an impression of negative control over the food[1]–which was predominantly evoked by high-calorie products–was accompanied by negative emotions (e.g., fear, disgust, guilt), while an impression of positive control over the food–which was mostly provoked by low-calorie items–was associated with positive emotions (e.g., happiness, safety).
A study conducted among college women emphasizes the importance of including the caloric value of food. Racine (2018) demonstrated that response towards high or low-calorie food images depended on different dimensions of dietary behaviors. More specifically, real decrease of food intake (i.e., dietary restriction) was associated with reduced pleasure responses towards both high and low-calorie food, while attempts to eat less or cognitive efforts to avoid eating (i.e., cognitive restraint) was associated to greater pleasure ratings for low-calorie food. Taken together, these results suggest that the caloric value of food might influence emotional reactions according to the type of restriction. Then, when examining ED individuals’ emotional reactions to food, it seems essential to include caloric value of food. In fact, there may be no difference in emotional rating of food between ED groups when the caloric value is not considered–like in Foroughi et al. (2018)’s experiment–but there may be some differences between AN and BN women if the energy content of foods is taken into account.
Finally, some studies have already yielded a better knowledge of the nutritional value of food in ED participants, in comparison to healthy women (Beumont et al., 1981; Laessle et al., 1988). As AN and BN individuals are concerned about their body appearance (weight, shape), they are likely interested in nutrition-related issues (American Psychiatric Association [APA], 2013; Robert-McComb et al., 2012). For instance, they can read extensive literature about nutrition to find new strategies to limit their food intake and/or to increase their caloric expenditure (Laessle et al., 1988). Some even consult fitness blogs and pro-ED websites (Mento et al., 2021: Mulveen & Hepworth, 2006; Rouleau & von Ranson, 2011; Rodgers et al., 2012). Given these elements, the idea that ED individuals may have better nutritional knowledge than the general population may be still relevant. Knowing that the more caloric the food is perceived, the more intense the negative reaction is likely to be (Gonzalez & Vitousek, 2004; Houben et al., 2010), it is relevant to believe that ED individuals’ nutritional knowledge can influence their emotional reactions to food. However, up until now, no study has examined the effects of objective ED women’s nutritional knowledge on their emotional responses to food[2], and no experiment has investigated for possible differences between AN and BN women about their knowledge.
The aim of the present study was to examine ED women’s emotional responses to food pictures, and to compare these responses according to their diagnosis, while taking into account both the caloric content of the food items presented and participants’ nutritional knowledge. Regarding emotional responses to food, we predicted that women suffering from an ED would present lower positive and higher negative reactions to food pictures than HC. Moreover, we hypothesized that AN participants would show more aversive reactions to food of low and medium energy density than BN women (APA, 2013). We also predicted that AN and BN women would have a better knowledge than HC about the energy content of the food depicted. Finally, we hypothesized that their knowledge would contribute to explain their unfavorable emotional responses to food, particularly for AN women.
meals (e.g., Gonzalez & Vitousek, 2004; Sunday et al., 1992), not on objective knowledge about food products (i.e., its accuracy).
Participants
Twenty-two women suffering from an ED and 22 HC women took part in the study. ED participants were recruited among outpatients of the Programme d'intervention des troubles des conduites alimentaires (PITCA) du Centre Hospitalier Universitaire (CHU) de Québec (n = 12), a multidisciplinary hospital unit for the assessment and treatment of ED, and among users of La masion l'Éclaircie services, a community-based organization for individuals presenting ED symptoms in Quebec city (n = 10). HC women were recruited among Laval University’s community by email advertisements (Mage = 23.41 ± 5.38 years; MBMI = 21.59 ± 2.25 kg/m2). In accordance with the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA, 2013), participants suffering from an ED were divided into two groups: the AN group (n = 13; Mage = 22.92 ± 3.99 years; MBMI = 18.91 ± 1.86 kg/m2) and the BN group (n = 9; Mage = 29.33 ± 9.68 years; MBMI = 25.96 ± 5 .79 kg/m2). Participants from the PITCA received their ED diagnosis from a psychiatrist specialized in ED (CR), while women from La Maison l'Éclaircie received theirs from a PhD student in psychology specialized in ED (CG), which was confirmed by an experienced clinical-researcher in the domain of ED (CB).
For the three groups, inclusion criteria were: a) being aged between 18 and 60 years old; b) understanding and speaking French; c) being right-handed; d) having normal or corrected-to-normal vision and audition; e) being free of drug and alcohol abuses for 3 months; f) presenting neither a psychotic disorder nor a neurological disorder; g) not showing any history of traumatic brain injury within the last 5 years; and h) not being pregnant. Furthermore, women of the HC group should not present: a) personal or family ED history; b) attempts to lose weight in the last month, and c) psychiatric disorders for which medications were prescribed and taken[1].
Procedure
Women suffering from an ED were tested in their usual health care setting, whereas HC were hosted at a research laboratory. All participants gave informed written consent prior to their participation. To reduce the influence of hungriness on tasks’ results[2], all participants were instructed to eat in the 60 minutes preceding their experimental session and were met at fixed hours (i.e. after breakfast, 8:30 am; or after lunch, 1:30 pm). The session lasted around 1.5 hour. First, women had to mention the time and the content of their preceding meal, estimate their level of appetite on a 7-point Likert scale (0 = I am not hungry; 6 = I am extremely hungry), and fill in questionnaires about their affective state (i.e., BDI-II, STAI-YA). Subsequently, they had to complete the emotional rating task of food and non-food pictures. A 10-min break was then taken considering the mental load associated to the first part of the session. Finally, participants performed the energy density ranking task of food pictures. They all received a monetary compensation of 14$CAD for taking part in the study. The experiment was approved by the Ethics Committee of the CHU de Quebec (Project 2012-8 12, C11-08-088).
Emotional rating
Participants were seated in front of a 16-inch LCD monitor connected to a PC, at a viewing distance of 60 cm. The room was dimly lit. The software E-Prime 2.0 Professional (Psychology Software Tools, Pittsburgh, PA, and Released 2012) was employed to create and administer the task. The food and object pictures were presented in a 700 x 526 pixels colored format, at the center of the screen, on a black font. The stimuli were shown for 5 seconds, one item at a time, in a random order. Not to influence the affective rating of pictures, their specific name or nature (e.g., “garlic pork sausage”, “pincers”) was not provided. When a food picture was presented, women were instructed to imagine, as vividly as possible, that they were eating the product/meal depicted (i.e., salient or intent-to-eat context; Murray & Strigo, 2018). When an object picture was displayed, they were asked to imagine themselves as using the item exposed or being in its presence. After each stimulus presentation, participants had to rate the emotions elicited by the item depicted on nine dimensions: valence, arousal, happiness/joy, sadness, anger, disgust, fear, surprise and neutrality. Women were not constrained by a limited amount of time, but they were told to share their immediate and instinctive emotional reactions towards the stimuli. For each picture, the last dimension to evaluate was followed by a short recovery period of 3 seconds, and then the next image to rate was presented. To reduce attentional errors and avoid participant’s confusion, the affective dimensions were always surveyed in the same order.
The valence and arousal levels of stimuli were investigated via Self-Assessment Manikin scales (SAM; Bradley & Lang, 1994; Lang, 1980), which are pictorials tools used for the measurement of a person’s affective response to stimuli. The SAM scales were depicted with a 9-point gradation, each character–and the space between two adjacent characters–corresponded to an ascending intensity level ranging from 1 (negative valence or low arousal) to 9 (positive valence or high arousal). For the remaining seven affective dimensions (i.e., happiness/joy, sadness, anger, disgust, fear, surprise and neutrality), Likert scales ranging from 1 (none) to 9 (very strongly), were used to assess emotions and the degree to which they experienced it. Ratings were collected by a numeric keypad. Before starting the task, in the presence of the experimenter (CG), participants made a practice trial with an object picture (i.e., a clock).
Energy density ranking
With all the stimuli in front of them, participants were instructed to rank the food from the lowest energy-dense (least kcal/g) to the highest energy-dense (most kcal/g), according to their knowledge. A dry-erase marker and a table-napkin were given to participants, so they could write on the pictures and correct their classification easily. When they were confident about their ranking, participants were invited to transcribe it on an answer form.
Screening of ED symptomatology.
Module H of the Structured Clinical Interview for DSM-IV-TRAxis I Disorders – Research version, Patient Edition (SCID-I/P; First et al., 2002), adapted for the DSM-5 criteria (APA, 2013), was used to diagnose ED. The SCID-I/P has an interjudge reliability of .70-1.0 and a test-retest reliability of .82-.90 for both clinical and community samples (First et al., 2002; Pike et al., 1995; Segal et al., 1994; Williams et al., 1992).
Diagnostic questions of the Eating Disorder Examination- Questionnaire (EDE-Q 6.0; Fairburn & Beglin, 2008) were used to validate the absence of significant ED manifestations in participants of the HC group. The instrument, requiring answers on 7-point Likert scales ranging from 0 (no day, not at all) to 6 (every day, markedly), addresses the core attitudinal features and behaviors of ED pathology over the past 28 days. To be included in the study as HC, women should not present fasting (score = 0) or important restrained eating to lose weight (score < 3 xss=removed xss=removed>r = .81-.94 for 2 weeks, r = .57-77 for about one year; Luce & Crowther, 1999; Mond et al., 2004b).
Assessment of participants’ comorbid affective state.
Depressive symptoms of participants were assessed by the Beck Depression Inventory II (BDI-II; Beck et al., 1996), a self-report questionnaire consisting of 21 items answered on a 4-point Likert scale ranging from 0 to 3 (example item: Crying; 0 = “I don’t cry any more than I used to”; 1 = “I cry more than I used to”; 2 = “I cry over every little thing”; 3 = “I feel like crying, but I can’t”). The BDI-II total score assesses respondents’ depressive mood in the past two weeks, with higher scores indicating more severe depressive symptoms. The questionnaire has a high internal consistency (α = .90) and a good test-retest stability (r =.73-.96; for review, see Wang & Gorenstein, 2013).
Anxiety symptoms of participants were assessed with the Part A of the
State-Trait Anxiety Inventory-Y Form
(STAI-YA, Spielberger, 1983). The STAI-YA measures State-Anxiety, which can be defined as feelings of apprehension, tension, nervousness and worry induced temporarily by situations perceived as dangerous. Twenty items, assessed on 4-point Likert scales, evaluate how respondents feel “right now” or felt “in a recent past” (example item: “I worry too much over something that really doesn’t matter”) A global score was computed by summing all items. Scores were then converted into an age-dependent T-score. The internal consistency of the whole inventory (Parts A and B) ranges from .86 to .95 and its test-retest reliability ranges from .31 to .86 (intervals fluctuating from 1 hour to 104 days; Gauthier & Bouchard, 1993; Spielberger, 1983).
Emotional rating task
Out of the 58 images displayed, 46 were food pictures and 12 were non-food pictures, i.e. object pictures (including one object picture used for a practice trial). Food pictures (n = 30) were chosen from the Institute of Nutrition and Functional Foods’ web-based food frequency questionnaire (Web-FFQ; Labonté et al., 2012), an online dietary assessment tool developed for qualifying and quantifying French Canadians’ dietary intakes using digital colored photographs of various food items and meals. The Web-FFQ was used to avoid potential limits and biases due to stimuli (Piqueras-Fiszman & Spence, 2014; Spence et al., 2016), because: a) its pictures are standardized in terms of viewing point, brightness, shading, background and cropping; b) its food products are presented with the same dinnerware and utensils, and 3) different portion sizes of food items and meals are available.
To maximise the diversity and the representativeness of food stimuli showed to women, some criteria guided the selection of the photographs: 1) the four main categories of Canada’s Food Guide (i.e., Vegetables and fruits, Grain products, Milk and alternatives, Meat and alternatives; Health Canada, 2011) and its “Other Foods” category (i.e., products that cannot be classified in the main categories, such as candies, chips, and pastries) had to be represented; 2) a reasonably comparable number of unprocessed and minimally-processed foods vs. moderately- and highly-processed foodstuffs had to be illustrated; 3) all food products had to be displayed on the same dinner plate, surrounded by the same fork and knife (i.e., beverages dispensed in a glass or a cup, and foods presented in a bowl were excluded); 4) the orientation and the localisation of the plate’s content had to be similar from one picture to another (i.e., pointing towards participants and in the middle of the plate, centered; Michel et al., 2015a,b; Rowley & Spence, 2018); 5) the plate’s area covered by foods had to be equivalent between stimuli minimally (Herzog et al., 2017; Kissileff et al., 2016); 6), the general nature of the food items and meals had to be easily identified or recognized (e.g., meat, cheese, pie); 7) based on past researches, foods for which positive and negative emotions could be evoked in ED and/or HC women had to be equally illustrated (e.g., strawberries, piece of cake, shellfish; Blechert et al., 2014; Charbonnier et al., 2016; Foroni et al., 2013; McNamara et al., 2008; Miccoli et al., 2016); and 8) low (< 1> 4.0 kcal/g) energy density foods had to be shown across the collection of images selected (Rolls & Barnett, 2000). Figure 1 shows examples of food stimuli used in the experiment’s tasks.

The object pictures were extracted from the International Affective Picture System (IAPS; Lang et al., 2008), a widely exploited database of images for the study of emotion. As for food stimuli, the selection of object pictures relied on specific criteria: 1) the objects had to be of common use or well-known; 2) they could not refer to foods, beverages or eating; 3) as much as possible, their size had to be similar from one picture to another, and to be equivalent to the portion size of food pictures previously chosen; 4) their background color had to be close to the one of food images (i.e., light gray beige). Moreover, according to the affective normative data of the IAPS (values on 9-point scales, ranging from 1 [negative or low] to 9 [positive or high]), the images must had: 1) a value between 4 and 6 on the Valence scale of Lang et al. (2008)’s data; 2) a value < 5>
Energy density ranking task
From the 46 food pictures used in the emotional rating task, 25 were picked up as stimuli for the energy density ranking task, which was designed to assess participants’ nutritional knowledge. The food pictures selected represented food items and meals easily found at local supermarkets. The food images were printed in a 8 x 6 cm colored format, on a US legal-size (21.6 x 35.6 cm) white paper. The stimuli were disposed in two columns of five pictures, totalizing three pages. The pages were laminated to facilitate their manipulation. The name, nature/flavor and cooking mode of the foods (e.g., “long-grain white rice, cooked”) were labelled under each stimulus.
All statistical analyses were carried out with SPSS 24.0 for Windows (IBM Corporation, Released 2016). All study variables were inspected for outliers and normality, and appropriate transformations were applied when needed. For all analyses, the alpha level, which was set to .05, was Bonferroni-corrected for multiple testing when required (i.e., decomposition of main effects and post-hoc comparisons). Univariate analyses of variance (ANOVAs) with post-hoc Tukey tests were performed to examine mean differences among AN, BN and HC groups on BMI, hungriness and scores on affective state (i.e., BDI-II, STAI-YA). Due to its fixed nature and its non-normal distribution, the mean age of groups was contrasted with non-parametric analyses, i.e. a Kruskal-Wallis test followed by Mann-Whitney U tests.
Emotional rating task
Participants’ ratings of food and object pictures were investigated according to the intensity of their emotional responses. For object pictures, a mean score including all object pictures pooled together was calculated for each emotional dimension and each group of participants surveyed (e.g., “Objects-Valence intensity-AN”). For food pictures, to examine whether women’s responses differed according to the energy density of the food displayed, the food stimuli were sorted in three classes, namely low (< 1> 4.0 kcal/g) energy density products (Rolls & Barnett, 2000). For each of these classes, each emotional dimension and each group of participants studied, an intensity mean score was computed (e.g., “Low energy density-Valence intensity-AN”).
In order to determine which variables to include in the group comparison analysis, Pearson correlations were run on the entire sample with emotional mean scores. Because valence, anger and sadness responses were strongly correlated together and with other emotional dimensions (r = .68 to .96), they were excluded from the analyses for the sake of parsimony. Surprise ratings were also excluded due to their lower relevance for the present study and their conceptual complexity (for review, see Mellers et al., 2013; Reisenzein et al., 2017). The remaining dimensions of arousal, happiness/joy, disgust, fear and neutrality were compared between AN, BN and HC groups using multivariate analyses of variance (MANOVAs). The decomposition of MANOVAs’ main effect (i.e., the multivariate one) was achieved with ANOVAs, then Tukey tests were used for post-hoc comparisons.
To test associations between women’s emotional responses and their comorbid affective state, correlation analyses were performed with reactions towards pictures and the STAI-YA scores. When variables were significantly related, the severity of anxiety symptoms was controlled for in the MANOVAs and ANOVAs. Because the STAI-YA and the BDI-II scores were strongly correlated (r = .86, p < .001), only the former was used as a covariate in the analyses. Finally, as the hunger level of women was not correlated with their emotional responses towards food and object pictures (all ps > .05), this variable was not entered as a covariate in the analyses concerning the stimuli-induced reactions.
Energy density ranking task
Participant’s performance on the energy density ranking task was assessed by means of a precision index, which was calculated by adding up the gap, in absolute value, between each food product’s real rank and the rank assigned. Thus, the higher the precision index was, the less accurate was women’s nutritional knowledge about the energy density of the items displayed. According to their real energy density value, the 25 food products were sorted out as low, medium or high-energy foods, and a precision index was computed for each class, for each participant. To explore the differences between groups on these three classes, a MANOVA was run. The anxious comorbid state was not controlled for in the analyses, because no association was found between participants’ precision indexes and their scores on the STAI-YA. For the same reason, the hunger level of women was not entered as a covariate in the analyses.
Finally, to verify if participants’ emotional responses to food pictures were explained by their nutritional knowledge, emotional ratings assigned to the 25 food products submitted in the ranking task were retrieved from the rating task’s results, and a mean score was calculated for each of the five affective dimensions investigated (i.e., arousal, happiness/joy, disgust, fear, and neutrality). Three multivariate multiple regression analyses (i.e., one per group) were then run to test whether the emotional ratings of food pictures (i.e., the intensity of reactions associated to them, on each dimension) would be predicted by the ranking task’s global precision index.
Group comparisons for age, BMI, hunger and comorbid affective state.
There were no significant differences between AN, BN and HC women for age, H(2, N = 44) = 4.49, p = .106, and for the level of hungriness preceding the experimental session, F(2, 41) = 1.25, p = .296. However, the groups differed on BMI, F(2, 41) = 16.78, p < .001, η2p =.45, BDI-II scores, F(2, 41) = 22.89, p < .001, η2p =.53, and STAI-YA scores, F(2, 41) = 29.48, p < .001, η2p =.59. More precisely, AN participants had a lower mean BMI than BN (p < .001) and HC women (p = .003), and BN participants had a higher mean BMI than HC (p = .007). For the comorbid affective state, AN and BN women showed more depressive (MAN = 22.15 ± 16.03; MBN = 16.67 ± 14.85; p < .001) and anxiety symptoms (MAN = 56.38 ± 11.96; MBN = 58.22 ± 14.59; p < .001) than HC did (MBDI-II = 2.64 ± 2.90; MSTAI-YA = 38.95 ± 5.40).
Emotional rating task.
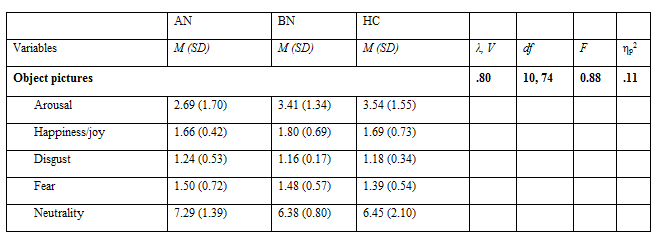
Object pictures.
For all object pictures, results showed a non-significant multivariate effect of Group (p = .560, see Table 1). Hence, no further analyses were achieved to examine the emotional dimensions.
Food pictures.
The MANOVA performed with low energy density food’ responses showed a significant multivariate effect of Group (p < .001; see Table 2). ANOVAs (α = .01) demonstrated a significant effect of Fear (p < .001, ηp2 = .63). According to post-hoc tests, AN and BN women judged low energy density food as more fearful than HC participants did (p < .001, p = .003). The AN group also reported higher ratings of fear than the BN group (p = .004). When controlling for anxiety symptoms (α = .01), the Fear effect remained significant (p < .001, ηp2 = .40), but the difference between BN and HC participants on that dimension was no longer statistically significant (p = .999).
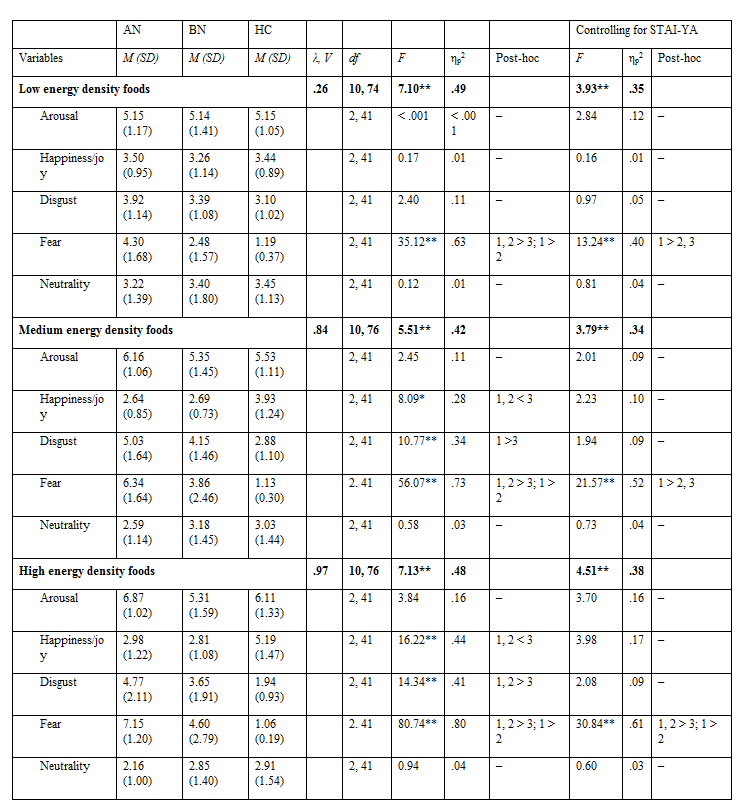
For medium energy density food, the results also indicated a multivariate effect of Group (p < .001), then ANOVAs (α = .01) showed significant effects for Happiness/Joy (p = .001), Disgust (p < .001) and Fear (p < .001) dimensions. The size of the effects found were high, particularly for the Fear dimension (ηp2 = .73). Post-hoc comparisons showed that the AN and BN groups had lower happiness/joy responses towards medium energy density foods than the HC one (p = .003, p = .014). Furthermore, AN women had greater disgust responses than HC (p < .001). For fear reactions, AN participants gave higher ratings than BN (p = .001) and HC (p < .001), and BN participants gave higher ratings than HC women did (p < .001). When controlling for anxiety symptoms (α = .01), the previously significant Happiness/Joy (p = .121) and Disgust effects were no longer significant (p = .157), but group differences remained on Fear (p < .001, ηp2 = .52), except the difference between the BN and HC groups which was no longer significant (p = .450).
The MANOVA conducted with high energy density food yielded a multivariate effect of Group (p < .001), and consecutive ANOVAs (α = .01) demonstrated significant univariate effects of Happiness/Joy (p < .001), Disgust (p < .001) and Fear (p < .001). Once again, the size of the effects found were high, particularly for the Fear dimension (ηp2 = .80). Post-hoc comparisons showed that AN and BN groups had lower happiness/joy responses (p < .001, p < .001), higher disgust responses (p < .001, p = .011) and greater fear reactions (p < .001, p < .001) to high energy density food than the HC group. In addition, AN women gave higher ratings of fear than BN participants did (p < .001). When controlling for anxiety symptoms (α = .01), the Happiness/Joy (p = .027) and the Disgust (p = .139) effects were no longer significant, but this time, the difference between BN and HC women on the Fear dimension remained significant (p = .013). The effect size of Fear also remained high, ηp2 = .61.
Energy density ranking task
Nutritional knowledge
The MANOVA ran with the precision indexes related to food’s classes of energy density did not show a significant multivariate effect of Group, indicating that AN, BN and HC women had a comparable nutritional knowledge, λ = .91, F(6, 78) = .61, p = .719, ηp2 = .05 (see Table 3).

Influence of nutritional knowledge on emotional responses to food pictures.
The results of the multiple regression analysis (α = .01) conducted for each group (i.e., AN, BN, and HC) showed that women’s nutritional knowledge about food products did not predict their arousal, happiness/joy, disgust, fear, and neutrality reactions towards them (all ps > .05). In other words, the intensity of participants’ reactions to food from the emotional rating task was not explained by their objective nutritional knowledge.
The objective of the present study was to examine ED women’s emotional responses to food pictures, and to compare these responses according to their diagnosis, while taking into account both the caloric content of the food items presented and participants’ nutritional knowledge. For this purpose, ED and HC women participated in an emotional rating task of food and object pictures, and an energy density ranking task of food items/meals. When appropriate, we controlled for the internal state of participants, that is their level of hungriness and their comorbid affective state, in order to reduce the effects of non-specific factors in the interpretation of results.
Emotional responses towards food and object pictures
Participants’ emotional responses according to food’s classes of energy density showed that when medium and high energy food were presented, groups clearly differed on the happiness/joy, disgust and fear dimensions, but when low energy items were displayed, only the fear dimension differed across groups. For AN and BN participants, higher fear reactions were observed compared to HC for all food pictures presented, regardless of their caloric value. AN women also experienced higher fear reactions than BN participants. In addition, the results showed that while AN participants judged medium and high energy density food as more disgusting than HC did, BN women’s disgust responses only exceeded those of HC for high energy food. Therefore, it seems that the caloric value of food necessary to generate disgust has to be higher with BN than with AN women. These findings are in line with those of Santel et al. (2006) and Rodriguez et al. (2007), which demonstrated respectively that AN and BN participants assessed images of high energy food as less pleasant than HC. They are also in accordance with the conclusions of Harvey et al. (2002) and those of Griffiths and Troop (2006), stating that women with high risk for ED rated images of high-density food as more disgusting than women at low risk. However, our findings extend those of previous research by distinguishing emotional responses of ED women to food based on their caloric value. They also support and extend the work of Racine (2018) conducted among college women, which revealed that an effective restriction (as seen in AN participants) is correlated with lower pleasure towards both high and low energy food, while temporary or infructuous attempts to eat less (as seen in BN participants) are associated to greater pleasure for low energy food. Such information is interesting for the development of therapeutic strategies targeting more efficiently patients’ cognitions and behaviors.
Regarding the analysis of object pictures, results showed that the three groups of participants did not differ in terms of intensity of their emotional ratings. The inclusion of non-food pictures allowed to verify if participants’ reactions were oriented exclusively towards food products or were explained rather by a global limited capacity to resent pleasure and/or a higher disgust sensitivity (see Aharoni & Hertz, 2012; Boehm et al., 2018; Deborde et al., 2006). The current results suggest that AN and BN participants’ negative reactions were oriented exclusively towards food. This finding supports the work of Davey et al. (1998) and Troop and al. (2002), which denoted that ED participants exhibit a higher disgust sensitivity for food and body-related stimuli, but not for other items. Consequently, it also refuted the hypotheses raised by some authors about the presence, in ED women, of a global lower disgust tolerance and a reduced general capacity to experience pleasure (Aharoni & Hertez, 2012; Boehm et al., 2018; Deborde et al., 2006).
Influence of participants’ internal state
The current study also aimed to control for women’s internal state. The methodological control we exerted for participants’ hungriness, i.e., instructions to eat 60 minutes prior to the experiment and meeting at fixed times of the day, was shown efficient because women’s appetite level before completing the tasks was low and did not differ between groups. Besides, the statistical control we applied for participants’ anxious state (which were highly correlated with their depressive symptoms) in the analysis of their emotional reactions towards food pictures modified the pattern of the results. Specifically, all group effects for happiness/joy and disgust responses that were demonstrated were no longer significant when controlling for anxious state. In other words, it seems that ED participants’ lower happiness/joy and higher disgust reactions towards food pictures were better explained by their anxiety state prior to the experiment. These results are consistent with those of Davey and Chapman (2009), which showed that controlling for anxiety overrides the association between disgust and ED-like symptoms. Accordingly, they postulated that the presence of anxious manifestations in individuals at risk of ED could amplify their experience of distress and negative emotions (e.g., disgust, displeasure) for sensitive stimuli. Building on these findings, anxiety state could have influenced their evaluation of food pictures by contributing to explain their aversive reactions towards them (e.g., less happiness/joy, more disgust).
Furthermore, regarding the fear effect, although it remained significant when controlling for anxiety state, the group differences observed between BN and HC women were no longer significant, except for the high-energy food category. These results contrast with those of Hay and Katsikitis (2014), which showed that ED women gave lower happiness and higher fear and disgust responses to food images than HC, even when their baseline level for these three emotions were controlled for. Nonetheless, the fact that the differences between BN and HC women were no longer significant when controlling for anxiety state on fear ratings for low and medium energy food, but remained significant for high energy food, is interesting. Patients’ sense of control towards food and the anticipation of consequences associated with food ingestion may explain these results. According to McNamara et al. (2008), when women suffering from an ED experience a feeling of loss of control over food, i.e. when they believe they cannot control their intake and their weight gain and/or their binge-purge behaviors, they may experience adverse emotions. Thus, it is possible that BN women thought they could manage their consumption of low and medium energy food because binge eating episodes mainly involve high sugar and fat products (Beumont, 2002; Gendall et al., 1997; Natenshon, 2009; Rosen et al., 1986). Therefore, food with lower energy value could have been considered at lower risk for inappropriate eating behaviors and potential weight gain. As a result, in the current study, the fear reaction to high-energy food was found to be more robust than fear reactions to lower energy food categories for BN participants.
For AN participants, their fear reactions were observed above and beyond their anxiety state prior to the experiment: the higher fear reactions observed among AN participants compared to HC and BN remained significant for all food energy density categories when controlling for participant’s anxiety state. Therefore, the relationship between AN diagnosis and fear reactions to food appears to be robust. These results suggest that AN participants might experience a negative sense of control and anticipated the consequences of food intake for all caloric classes of food. This hypothesis relies on the idea that a core manifestation of AN is a morbid fear of gaining weight or becoming fat (APA, 2013). Then, even for low and medium energy food, women with AN could apprehend gaining some weight (or not maintaining their actual low weight) if they ingest them, as if all foods, independently of their caloric content, could represent a serious self-directed threat (Milos et al., 2017; Paslakis et al., 2016; Steinglass et al., 2007).
Nutritional knowledge and its impact
The results of the ranking task revealed that AN and BN women did not have better nutritional knowledge than HC about the energy density value of everyday food products. The three groups showed similar results when ranking food according to their caloric value. Furthermore, the results revealed that participants’ nutritional knowledge, as we measured it, did not have a significant influence on their emotional responses; no association was found between women’s nutritional knowledge and emotional reactions to food, regardless of their diagnosis. Therefore, it appears that ED participants’ aversive reactions towards foods were not explained by their objective knowledge of caloric content. Instead, their emotional reactions may be influenced by their implicit cognitions about food and their subjective perception of food items’ energy content, which seems to be erroneous (Eiber et al., 2005; Gonzalez & Vitousek, 2004; Provencher et al., 2009; Sunday et al., 1992; Vartanian et al., 2004).
These findings leaded to the rejection of our hypotheses regarding nutritional knowledge, but the latter were mainly based on experiments held in the 1980s, at which time food and nutrition information was not as omnipresent in the public area as it is today (i.e., Beumont et al., 1981; Laessle et al., 1988). Nowadays, nutritional information is more abundant, elaborate, and readily available to the general population. It is possible that such a new social context has contributed to reduce the gap between HC and ED’s nutritional knowledge about foods’ energy value (Breen & Espelage 2004; Soh et al., 2009).
Strengths and limitations
To our knowledge, this study is the first to explore ED participants' emotional responses to food according to their diagnosis and to the caloric content of the food products presented, while considering their comorbid affective state. Other strengths of the present study rely on the statistical control for participants' appetite level and on the investigation of the impact of their nutritional knowledge on their emotional reactions to foods. Furthermore, our experiment used a collection of standardized food pictures, which allowed to reduce the potential biases associated with different visual parameters, increasing the internal validity of our experiment. It should be noted that the set of food pictures used in this experiment (and their affective ratings) represents one of the first databases conceived for the examination of food-induced emotions in North-American ED individuals, most of those already available having been developed in Europe (e.g., FoodCast research image database, Foroni et al., 2013; Full 4 Health Image Collection, Charbonnier al., 2016; Open Library of Affective Foods; Miccoli et al., 2014, 2016). Thus, our bank of culturally representative food pictures could contribute to the development of clinical advances for North-American ED populations.
Despite its strengths, the present experiment has some limitations that must be mentioned. First, the fact that ED women, especially AN participants, may not be classified as critically ill as revealed by their outpatient status and their mean BMI outside the underweight category (i.e., > 18.5 kg/m2). However, even if their illness’s severity can appear to be low according to theses clinical aspects, the AN and BN participants of our study suffered from clear and significant ED symptoms, as assessed by a structured interview (i.e., module H of the SCID-I/Pl) and a specialized questionnaire (i.e., EDE-Q 6.0). Second, the absence of non-neutral non-food images—i.e., of pictures that could have evoked low happiness/joy and high disgust or fear responses like the food ones did−represents another limitation. The inclusion of such stimuli could have certified even more the specificity of food pictures in the induction of aversive reactions in ED women. Nevertheless, the inclusion of object images partially contributed to demonstrate this point. Third, the ranking task of food items according to their energy density to measure participants' nutritional knowledge may have been too difficult. This could have lowered their performance and reduced the probability to find differences between groups. Indeed, the task involved ranking many food products and some of them had a fairly similar caloric content. Finally, the representativeness of food’s energy density as a measure of participants' nutritional knowledge can be discussed, as this element focuses on only one aspect of this knowledge. Consequently, the use of another type of nutritional knowledge measure–e.g., a questionnaire as those elaborated by Klieman et al., 2016; Saarela et al., 2013; and Dickson-Spillmann et al., 2011–could have been more relevant given the purpose of its inclusion.
This study demonstrated that ED women experienced a high level of fear towards food pictures, which was neither due to their level of hungriness nor to their affective comorbid state. This fear response appeared to be specific to food, because no difference between participants’ emotional responses was noticed for object pictures. Most importantly, the study takes the literature further in the field of ED by revealing clear distinctions in women’s reactions according to their diagnosis and according to the caloric content of the food presented. Precisely, for all food products displayed, regardless of their energy density, AN participants showed a more intense reaction of fear than BN and HC. However, only high-calorie items led to a higher fear response in BN participants than in HC, irrespectively of their anxiety state prior to the experiment. These results underline the necessity for treatments to address explicitly ED women’s fear towards common food items and meals in a way of ensuring a long-term reduction of their symptoms and their recovery. In this perspective, our results support the use of therapeutic techniques that have been shown to be valid for anxiety disorders (e.g., gradual exposure and response prevention) in order to increase the effectiveness of psychological treatment of AN and BN (Levinson et al., 2014; Reilly et al., 2017; Steinglass et al., 2011; Treasure et al., 2015; Webb et al., 2011). Finally, the study revealed that participant’s aversive reactions towards food pictures were not caused by their objective nutritional knowledge about them, which suggests that implicit cognitions might rather modulate their emotional responses. In summary, the study highlighted the key role of food-induced fear in ED’s symptomatology, particularly in AN, and stressed the necessity of implementing treatments that address it exhaustively in order to improve patients’ eating behaviors.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti
