AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2642-9756/131
1 RN Nure midwife, Nurse Manager, Nursing department. Armed Forces Hospital Southern Region, Khamis Mushait 62481 Saudi Arabia.
2 Professor Maternal and Child Health Nursing Department, College of Nursing.
*Corresponding Author: Halimah Alshahrani, RN Nure midwife, Nurse Manager, Nursing department. Armed Forces Hospital Southern Region, Khamis Mushait 62481 Saudi Arabia.
Citation: Halimah Alshahrani, Juliana Linnette D’Sa. (2023) Effectiveness of Single -Use Hot Pack on Labour Pain, Duration of Labour, and Satisfaction of Primigravida: A Randomised Controlled Trial. J. Women Health Care and Issues. 6(1); DOI:10.31579/2642-9756/131
Copyright: © 2023 Halimah Alshahrani, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 October 2022 | Accepted: 09 December 2022 | Published: 04 January 2023
Keywords: heat therapy; hot packs; labour pain; duration of labour; satisfaction
Background: Labour pain is a highly individualized experience. Although heat influences labour pain, duration and maternal satisfaction, evidence on the effectiveness of single-use instant hot packs is scare.
Objectives: To examine the effect of hot pack applied on the lower back of primigravid women in the active phase of labour on pain intensity and labour duration and to determine satisfaction with the labour and delivery experience.
Methods: A randomised controlled trial was conducted in Armed Forces Hospital with Primigravidae in the active phase of labour. Participants were randomly selected and assigned to the intervention group (n = 45) and the control group (n = 46). The intervention group received an application of hot pack on the lower back for 30 min, followed by rest for 10 min; the cycle was continued until birth of the fetus. The control group received routine care, that also included intermittent Entonox inhalation.
Finding: Of the 91 women, those who received hot packs had significantly lower labour pain intensity score at all assessment points (30, 60, 90, 120, 150, and 210 min) than women in the control group (p≤0.05). The duration of labour did not differ significantly between the two groups (p≥0.05). The intervention group had significantly higher satisfaction scores with the labour and delivery experience than the control group (p≤0.05).
Conclusions: The hot pack is an effective nonpharmacologic method for reducing pain intensity during labour and provides women an overall satisfactory labour and delivery experience although ineffective in shortening the duration of labour.
Labour pain is a highly individualized experience, and its role has been established [1]. Described as the most significant source of discomfort for women in labour, the perception of pain is highly variable [2] and often exceeds endurance levels. Pain, one of the key elements of childbirth fear[3], is a common concern of first-time mothers [4]. To ensure a satisfying childbirth experience, effective pain control is critical [5]. If inappropriately managed, pain can adversely affect both the woman and her fetus6 and influence the labour and delivery experience. Pain relief gives women control and enables them to participate in the childbirth experience [7]. Most women prefer to use pain relief measures during labour. More than half (60%) of the women surveyed in a Saudi Arabian study, expressed their preference for pain relief measures [8]. Both, pharmacological or non-pharmacological measures to relieve labour pain are available. Nitrous oxide (N2O) is among the widely used pharmacological measures, although evidence regarding it’s analgesic effect is limited [9]. Most studies comparing it with other agents shows heterogeneous results regarding its effect on labour pain relief [10,11,12]. Although pharmacologic measures are known to have maternal and fetal side effects [13], it is used in most setting. Some women routinely ask for intermittent Entonox inhalation and discontinue its use abruptly on experiencing side effects.
Increasing number of women seek non-pharmacologic interventions of pain relief because of the minimal side effects compared to medications and other therapies [14]. Evidence shows that heat reduces labour pain intensity. Heat works on the principle of the gate control theory of pain. Melzac and Katz (1994), as cited [15], It increases blood flow, tissue metabolism, and connective tissue elasticity, leading to inhibition of the pain receptors’ transmission to the brain. It stimulates heat receptors in the skin and deep tissue, causing the impulses to balance themselves at the spinal cord, thereby closing the gate of pain impulses from reaching the brain [16]. When calcium channels in the spinal cord are activated, pain receptor activity is inhibited [17]. Evidence shows that warm compresses [18,19], hot water bottles [20], warm bags [21], and warm showers [7,22,23] applied to different body sites were effective in reducing labour pain. However, a systematic review [24], concluded that the evidence on pain relief was of very low uncertainty, stating that only three of the trials were of good quality.
Although heat increases uterine contractility and may shorten the duration of labour, there is lack of evidence about it’s effectiveness [25] with most studies reporting inconsistent findings. In a comparison with routine care, reported significantly shorter duration of the first and third stages of labour on applying heat to the lower back for 80 min and to the perineum for 5 min, with no difference in the second stage of labour [26]. Researchers found no difference in the duration of labour although it was effective in pain relief [21]. Although some studies had robust methodology such as clinical trials [17,19,22,26], others lacked randomization [19], resulting in inconsistent findings. For women to experience a meaningful childbirth experience, it is essential to manage labour pain. Women who experience less labour pain have higher satisfaction with the labour experience [3,27]. Further, a shorter duration of pain and suffering, has an influence on the satisfaction with childbirth experience [19].
Although a variety of pain relief methods are used, pain management during labour remains a serious topic for obstetricians and midwives alike [16]. There is limited use of non-pharmacological pain relief measures in Saudi Arabia because of the specific regulations and policies of the hospitals, lack of knowledge among health care providers, and women’s unwillingness to use nonpharmacologic treatments [28].
Midwives play a crucial role in providing comfort to women in labour. Assessing the physical and emotional state of women and helping them cope with pain are important aspects of caring [29]. Effective pain management encourages women to seek normal vaginal delivery and to have a positive and satisfying childbirth experience. Single-use hot packs tends to be simple and easy women can use and still maintain control during labour. It does not require intense training for nurses to use it for pain management. Although heat may reduce pain and may have an effect on the duration of labour, the effectiveness of single use hot packs remains is not known. Heat from the hot pack is generated by squeezing it between the palms of the hand to activate the prefilled magnesium sulphate and water. Therefore, we examined the efficacy of instant single-use hot packs during active phase of first stage of labour in reducing labour pain intensity and labour duration in comparison with routine care. We also examined the satisfaction of the women with the labour and delivery experience.
2.1 Study Design
We conducted this randomised controlled trial between August 2018 and July 2019. Participants were randomised to one of two arms: an intervention group (single-use instant hot packs; Dynarex) and a control group (routine care, including the use of intermittent Entonox inhalation).
2.2 Participants and setting
Participants were recruited by the first author from the labour and delivery unit of Armed Forces hospital Southern Region. Women were included in the study if they met the criteria: primigravid, had normal onset of labour after a normal term pregnancy (>37-42 weeks of gestation), in the active phase of the first stage of labour with 6-8 cm cervical dilatation. Women were excluded if they had fever, skin infection, eczema, injury or inflammation of the back, bleeding, deep vein thrombosis, edema, other high risk complications, medical conditions, decreased fetal movement, intrauterine growth restriction, intrauterine fetal death, and history of infertility.
Using G power software (version 3.0.10), we calculated the sample size using two-tailed tests. A total of 90 participants, with 45 participants per arm, was required to achieve a power of 80% with an error probability of 5% and an effect size of 0.3. We assessed eligibility of 138 participants: assuming approximately 10% attrition rate, we recruited 100 participants. Initially, 50 participants were randomly allocated to intervention group and an equal number in the control group. Five participants were excluded from the intervention group because of emergency CS (n = 3), Entonox administration on request (n = 1), or received an injection of pethidine (n = 1). In the control group four were excluded because of emergency CS (n = 2) or induction of labour (n = 2). The final sample consisted of 91 participants, with 46 in the intervention group and 45 in the control group. The consort flow diagram in Figure 1 presents the participants’ passage through each group.

Figure 1: CONSORT flow diagram. Participants’ passage through each group.
2.3 Randomisation
The hospital records were assessed to determine the eligibility of the women to participate; they were randomly allocated to the intervention group (single-use instant hot pack) or control group (routine care including use of intermittent Entonox) using a computer-generated block randomisation sequence that involved a block size of two. Blinding was not possible due to the nature of the intervention.
2.3.1 Intervention
The intervention consisted of application of single-use hot packs on the women’s lower back for 30 minutes followed by 10 minutes period of rest, and the cycle was continued until delivery. The hot pack (Dynarex, first voice, disposable instant hot pack measuring 5X9 inches, that contained magnesium sulfate and water had approval from the US Food and Drug Administration). It was activated by squeezing it from the outer edges toward the center and applying friction with the palms of the hands. To ensure intervention fidelity, the temperature of the physical environment was maintained between 22°C and 24°C.
2.3.2 Control
The control group received routine care that included monitoring of general well-being, uterine contractions, vaginal examination, cardiotocography monitoring, intravenous fluid administration, oxygen administration if needed, enema, catheterization, and appropriate nursing care. As per the protocol of the labour and delivery unit, women received optional intermittent Entonox inhalation for labour pain management. Entonox consisted of premixed 50% Oxygen and 50% Nitrous Oxide in a cylinder and was inhaled via a facemask, the women took a deep breath via Entonox mask during contractions and to breath normally without Entonox between the contractions. Women in the control group were observed by the researcher until birth.
2.4 Ethical considerations
The Research ethical committee of XXX approved the study on April 2018 (XXX Administrative approval was provided by the Head of the Labour and Delivery Unit. Written informed consent was taken from participants, who also had the right to withdraw without consequences. Confidentiality and privacy were maintained throughout the study.
2.5 Data collection
Eligible women who were randomly allocated to the intervention group received verbal information about the hot pack application, the voluntary nature of the study and the right to withdraw without any consequences and they signed the consent form. At baseline, demographic data that included maternal age, education, employment status, family type, family income, and physical characteristics (height and weight) were collected through interview. Obstetrical data that included gestational age, characteristics of uterine contractions, and cervical assessment were gathered from the participant’s hospital records and entered in a record analysis sheet.
The outcome measure labour pain intensity was assessed using the visual analogue scale (VAS) for pain intensity and the duration of labour was assessed with the partograph [30]. The extensively used valid and reliable VAS consists of a horizontal line with a marking 0 cm (no pain) to 10 cm (worst or intolerable pain). Participants assigned scores on the VAS based on their perception of labour pain intensity at baseline then every 30 minutes intervals until the delivery. The test–retest reliability (0.71–0.94) and a correlation coefficient (r=0.79–0.96) when compared with common pain measures [31] provided evidence of the scale reliability. The WHO-modified partograph [32]. has graphical information of fetal condition, progress of labour, and maternal condition: fetal heart rate, liquor, cervical dilatation, descent of the presenting part, and uterine contractions. The duration of labour was computed using the data from the partograph. The satisfaction of the women with the labour and delivery experience was measured 2 hours after delivery using an author-developed, 13-item, five-point Likert-type Labour and Delivery Satisfaction Scale (LDSS). Responses were rated as 1 = very dissatisfied, 2 = dissatisfied, 3 = neither satisfied nor dissatisfied, 4 = satisfied, and 5 = very satisfied. The score ranged from 13–65, with a higher score indicating greater satisfaction. Items were developed based on literature and specifically consulting a previous study [33]. Five experts (four faculty with maternity nursing specialization and one clinical practitioner with an obstetrical and gynecology specialty) validated the English version of the scale. Items were retained if 80% of the experts agreed on the relevance. After modification, it was translated to the Arabic language and back-translated to English by a language expert to ascertain language validity. After pretesting the instrument, two items were modified to improve clarity. The scale was reliable (alpha = 0.846). Participants took 5 minutes, on an average, to complete the scale. One item, “Overall satisfaction,” gave participants the opportunity to provide a global rating of their satisfaction. They did not respond to the open -ended item “any other comments.”
The control group received routine care that also included optional Entonox inhalation. All measurements were done similar to that of the intervention group. Prior to data collection, a pilot study on a different sample of 10 women ensured feasibility of the study.
1.Statistical analyses
Data were analysed using IBM Statistical Package for Social Sciences (version 20.0). The frequency and percentage for categorical data and the mean and standard deviation for continuous variables were computed. Independent t tests were used to analyse normally distributed continuous variables. Mann–Whitney U and Fisher’s exact test were applied to data that were not normally distributed. A two-tailed P value was set at an alpha level of 0.05 and confidence interval was computed.
2.3 Randomisation
The hospital records were assessed to determine the eligibility of the women to participate; they were randomly allocated to the intervention group (single-use instant hot pack) or control group (routine care including use of intermittent Entonox) using a computer-generated block randomisation sequence that involved a block size of two. Blinding was not possible due to the nature of the intervention.
2.3.1 Intervention
The intervention consisted of application of single-use hot packs on the women’s lower back for 30 minutes followed by 10 minutes period of rest, and the cycle was continued until delivery. The hot pack (Dynarex, first voice, disposable instant hot pack measuring 5X9 inches, that contained magnesium sulfate and water had approval from the US Food and Drug Administration). It was activated by squeezing it from the outer edges toward the center and applying friction with the palms of the hands. To ensure intervention fidelity, the temperature of the physical environment was maintained between 22°C and 24°C.
2.3.2 Control
The control group received routine care that included monitoring of general well-being, uterine contractions, vaginal examination, cardiotocography monitoring, intravenous fluid administration, oxygen administration if needed, enema, catheterization, and appropriate nursing care. As per the protocol of the labour and delivery unit, women received optional intermittent Entonox inhalation for labour pain management. Entonox consisted of premixed 50% Oxygen and 50% Nitrous Oxide in a cylinder and was inhaled via a facemask, the women took a deep breath via Entonox mask during contractions and to breath normally without Entonox between the contractions. Women in the control group were observed by the researcher until birth.
2.4 Ethical considerations
The Research ethical committee of XXX approved the study on April 2018 (XXX Administrative approval was provided by the Head of the Labour and Delivery Unit. Written informed consent was taken from participants, who also had the right to withdraw without consequences. Confidentiality and privacy were maintained throughout the study.
2.5 Data collection
Eligible women who were randomly allocated to the intervention group received verbal information about the hot pack application, the voluntary nature of the study and the right to withdraw without any consequences and they signed the consent form. At baseline, demographic data that included maternal age, education, employment status, family type, family income, and physical characteristics (height and weight) were collected through interview. Obstetrical data that included gestational age, characteristics of uterine contractions, and cervical assessment were gathered from the participant’s hospital records and entered in a record analysis sheet.
The outcome measure labour pain intensity was assessed using the visual analogue scale (VAS) for pain intensity and the duration of labour was assessed with the partograph [30]. The extensively used valid and reliable VAS consists of a horizontal line with a marking 0 cm (no pain) to 10 cm (worst or intolerable pain). Participants assigned scores on the VAS based on their perception of labour pain intensity at baseline then every 30 minutes intervals until the delivery. The test–retest reliability (0.71–0.94) and a correlation coefficient (r=0.79–0.96) when compared with common pain measures [31] provided evidence of the scale reliability. The WHO-modified partograph [32]. has graphical information of fetal condition, progress of labour, and maternal condition: fetal heart rate, liquor, cervical dilatation, descent of the presenting part, and uterine contractions. The duration of labour was computed using the data from the partograph. The satisfaction of the women with the labour and delivery experience was measured 2 hours after delivery using an author-developed, 13-item, five-point Likert-type Labour and Delivery Satisfaction Scale (LDSS). Responses were rated as 1 = very dissatisfied, 2 = dissatisfied, 3 = neither satisfied nor dissatisfied, 4 = satisfied, and 5 = very satisfied. The score ranged from 13–65, with a higher score indicating greater satisfaction. Items were developed based on literature and specifically consulting a previous study [33]. Five experts (four faculty with maternity nursing specialization and one clinical practitioner with an obstetrical and gynecology specialty) validated the English version of the scale. Items were retained if 80% of the experts agreed on the relevance. After modification, it was translated to the Arabic language and back-translated to English by a language expert to ascertain language validity. After pretesting the instrument, two items were modified to improve clarity. The scale was reliable (alpha = 0.846). Participants took 5 minutes, on an average, to complete the scale. One item, “Overall satisfaction,” gave participants the opportunity to provide a global rating of their satisfaction. They did not respond to the open -ended item “any other comments.”
The control group received routine care that also included optional Entonox inhalation. All measurements were done similar to that of the intervention group. Prior to data collection, a pilot study on a different sample of 10 women ensured feasibility of the study.
1.Statistical analyses
Data were analysed using IBM Statistical Package for Social Sciences (version 20.0). The frequency and percentage for categorical data and the mean and standard deviation for continuous variables were computed. Independent t tests were used to analyse normally distributed continuous variables. Mann–Whitney U and Fisher’s exact test were applied to data that were not normally distributed. A two-tailed P value was set at an alpha level of 0.05 and confidence interval was computed.
1.Results
3.1 Baseline characteristics of participants
A total of 100 women were randomly allocated at first, 50 each in the intervention and the control groups. Five women from the intervention group and four women from the control group were excluded because of attrition (n=9, attrition rate =9.9%). Finally, 45 women from the intervention group and 46 from the control group were included in the study. No statistically significant difference was observed in the demographic and obstetrical data when the two groups were compared at baseline (p > 0.05) Table 1 presents the findings.
| Variables | Total (n=91) | Intervention group (n=45) | Control group (n=46) | P value |
| Maternal age (y), mean (SD) | 25.4 (4.64) | 25.2 (4.27) | 25.5 (5.01) | 0.778b |
Educational level, no. (%) ≤ High school Graduate |
44 (48.4) 47 (51.6) |
25 (55.5) 20 (44.4) |
19 (41.3) 27 (58.7) | 0.104a |
Employment, no. (%) Yes No |
3 (3.3) 88 (96.7) |
2 (4.4) 43 (95.6) |
1 (2.2) 45 (97.8) | 0.617a |
Family income (SR);1 SR = 3.75 $US), no. (%) < 5000> 5000–10000 >10000 |
7 (7.7) 65 (71.4) 19 (20.9) |
6 (13.3) 31 (68.9) 8 (17.8) |
1 (2.2) 34 (73.9) 11 (23.9) | 0.122a |
| Height (cm), mean (SD) | 153.7 (5.85) | 153.9 (5.48) | 153.6 (6.23) | 0.779b |
| Weight (kg), mean (SD) | 66.3 (10.9) | 65.7 (10.6) | 66.9 (11.3) | 0.610b |
| Gestational age (w), mean (SD) | 38.8 (1.03) | 39.0 (.929) | 38.7 (1.10) | 0.191b |
Uterine contraction Frequency, no. (%) ≤ 3 in 10 min 4–5 in 10 min Intensity, no. (%) Moderate Strong |
73 (80.2) 18 (19.8)
43 (47.3) 48 (52.7) |
34 (75.6) 11 (24.4)
19 (42.2) 26 (57.8) |
39 (84.8) 7 (15.2)
24 (52.2) 22 (47.8) |
0.386a
0.347a
|
Duration (sec), mean (SD) Interval (min). mean (SD) | 57.2 (7.06) 2.00 (.494) | 56.6 (6.30) 1.98 (.543) | 57.6 (7.76) 2.02 (.447) | 0.499b 0.674b |
Cervical assessment Dilatation (cm), mean (SD) Effacement (%), mean (SD) |
6.62 (.928) 77.4 (7.58) |
6.67 (.953) 76.4 (7.73) |
6.61 (.930) 78.2 (7.39) |
0.770b 0.255b |
Presenting part station, no, (%) (- 3) (- 2) (- 1) (0) Membranes’ status, no, (%) Intact Ruptured |
22 (24.1) 48 (52.8) 14 (15.4) 7 (7.7)
19 (20.9) 72 (79.1) |
14 (31.1) 23 (51.1) 5 (11.1) 3 (6.7)
11 (24.4) 34 (75.6) |
8 (17.4) 25 (54.3) 9 (19.6) 4 (8.7)
8 (17.4) 38 (82.6) | 0.138a
0.414a
|
Abbreviation: (n) Sample size, (y) Years, (SD) Standard Deviation, (%) Percentage, (SR) Saudi Riyals, (cm) Centimeter, (kg) Kilograms, (w) Weeks, (sec) Seconds, (min) Minutes.
aFisher exact test.
bIndependent-samples t test, p ≤ 0.05
Table 1. Comparison of baseline characteristics between intervention and control group
Among the 91 women who completed the study, the mean age was 25.4 (SD = 4.64) years, and 51.6% had a college education. Most of them (96.7%) were unemployed, and 71.1% had a monthly family income of 5000–10000 Saudi Riyals (approximately one Saudi Riyal = 3.75 $US). The mean gestational age of the women was 38.86 (SD = 1.03) weeks; most (80.2%) had ≤three uterine contractions in 10 min, and the mean duration of the contractions was 57.2 (SD = 7.06) seconds. The mean interval between uterine contractions was 2 min (SD = 0.494). It was determined that the mean cervical dilatation was 6.62 (SD = 0.928) cm, and mean effacement was 77.4% (SD =7.58); the fetal head of 52.8% was at -2 station and the membranes were ruptured in 79.1% of the women. These obstetrical data were not statistically different between the intervention and control group (p > 0.05).
3.2 Labour pain intensity
We hypothesized that the application of single-use instant hot packs on the lower back of primigravid women in the active phase of labour would significantly reduce the mean labour pain intensity scores as compared with that of the controls (H1). At baseline, the mean pain intensity scores of the intervention group (8.02; SD = 0.84) and control group (8.07; SD = 0.95) were not statistically different (p = 0.820, 95%, CI= 0.331, −0.417). After the intervention, the mean pain intensity scores at all measurement points (30, 60, 90, 120, 150, 180, and 210 min) were significantly lower compared to the control group. After 30 min (p ≤ 0.05, CI: −0.775,−1.913) and 60 min measurement points (p ≤ 0.05, CI:−0.707,−1.760), the sample size decreased as the women transitioned from the active stage of labour to complete dilatation and delivery (at 90 min n= 43, at 120 min n= 34, at 150 min n= 24, at 180 min n= 21 and at 210 min n=15) (Figure 2). However, there was a significant decrease in the measurement points at 90 min (p ≤ 0.05, CI: −0.839 to −1.859), 120 min (p ≤ 0.05, CI: −0.833 to −1.886), 150 min (p ≤ 0.05, CI: −0.435 to −1.502). 180 min (p ≤ 0.05, CI: −0.751 to −1.916) and 210 min (p ≤ 0.05, CI: −0.933 to −2.314), showing the efficacy of the hot pack in decreasing the intensity of labour pain (Table 2).
| Assessment periods | Intervention Group Mean, (SD) | Intervention Group n (%) | Control Group Mean, (SD) | Control Group n (%) | t-test | P value | 95% Confidence Interval |
| At baseline (T0) | 8.02, 0.84 | 45 (100) | 8.07 ± 0.95 | 46 (100) | −0.228 | 0.820 | 0.331 to -.417 |
| At 30 Min (T1) | 6.18 ± 1.41 | 45 (100) | 7.52 ± 1.31 | 46 (100) | −4.693 | 0.000* | −0.775 to −1.913 |
| At 60 Min (T2) | 6.27 ± 1.38 | 45 (100) | 7.50 ± 1.13 | 46 (100) | −4.652 | 0.000* | −0.707 to −1.760 |
| At 90 Min (T3) | 6.49 ± 1.31 | 43 (96) | 7.84 ± 1.04 | 43 (93) | −5.263 | 0.000* | −0.839 to −1.859 |
| At 120 Min(T4) | 6.41 ± 1.10 | 34 (76) | 7.77 ± 1.08 | 35 (76) | −5.154 | 0.000* | −0.833 to −1.886 |
| At 150 Min (T5) | 6.79 ± 1.02 | 24 (53) | 7.76 ± 0.831 | 25 (54) | −3.649 | 0.001* | −0.435 to −1.502 |
| At 180 Min (T6) | 6.67 ± 1.01 | 21 (47) | 8.00 ± 0.873 | 22 (48) | −4.621 | 0.000* | −0.751 to −1.916 |
| At 210 Min (T7) | 6.73 ± 1.03 | 15 (33) | 8.36 ± 0.745 | 14 (30) | −4.825 | 0.000* | −0.933 to −2.314 |
*Independent-samples t test, significance level at p ≤ 0.05.
Table 2: Comparison of labour pain intensity scores between the intervention and control group
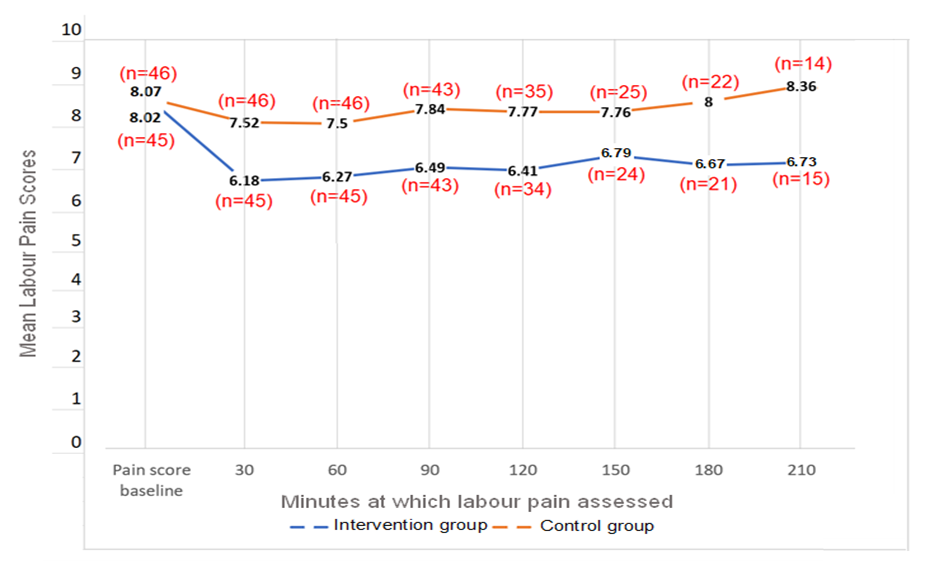
Figure 2: Mean labour pain scores with sample size in the intervention and control groups
3.3 Duration of labour
We hypothesized that the application of single -use hot packs to the lower back of women in the active phase of labour would significantly reduce the mean duration of labour as compared with the controls (H2). The overall mean labour duration in the intervention group (7.5 hours /451.5 min; SD = 162.2 min) was shorter than that of the control group (7.8 hours/467.3 min; SD = 155.2 min). However, the difference was not statistically significant (p = 0.617), In addition, there was no statistical difference in the mean duration of the first, second and third stage of labour between the groups. (P > 0.05), indicating that the hot pack application was not effective in shortening the duration of labour (Table 3).
| Duration of Labour Stages (in min) | Intervention group n = 45 | Control group n = 46 | Z Score | P value |
| Mean± Standard Deviation | Mean± Standard Deviation | |||
| First Stage | 418.8 ± 152.7 | 436.6 ± 155.5 | -.512 | 0.608 |
| Second Stage | 26.1 ± 24.1 | 29.3 ± 27.2 | -.636 | 0.525 |
| Third Stage | 5.4 ± 1.2 | 5.6 ± 2.1 | -.379 | 0.704 |
| Total labour duration | 451.5 ± 162.2 | 467.3 ± 155.2 | -.500 | 0.617 |
*Mann–Whitney U test, significance level at p ≤ 0.05.
Table 3: Comparison of the Duration of Labour in the Intervention and Control Groups
3.4 Satisfaction with labour and delivery experience
The women in the intervention group had significantly higher overall mean satisfaction score (p= .000) compared to the control group. Their mean score was significantly higher on all items, except the satisfaction regarding the “happiness with the care received” and “labour and delivery experience,” were not significantly different between the groups (p = 0.918 and 0.257, respectively) (Table 4)
| Satisfaction Scale | Intervention group n = 45 | Control group n = 46 | Z Score | P value |
| Mean± Standard Deviation | Mean± Standard Deviation | |||
| I'm satisfied with the method of pain relief | 4.56 ± .546 | 3.91 ± .985 | −3.55 | .000* |
| I'm satisfied with the level of pain relief | 4.53 ± .694 | 3.65 ± 1.016 | −4.80 | .000* |
| I'm satisfied because I have no side effects of the pain management methods | 4.69 ± .596 | 4.04 ± .868 | −4.03 | .000* |
| I felt happy about the care I received | 4.49 ± .549 | 4.41 ± .748 | -.103 | .918 |
| I felt happy about labour and delivery experience | 3.44 ± 1.078 | 3.26 ± 1.084 | −1.13 | .257 |
| My wishes were always respected | 4.42 ± .839 | 4.07 ± .879 | −2.30 | .021* |
| The staff gave me sufficient information about my progress | 4.69 ± .701 | 4.35 ± .674 | −3.07 | .002* |
| The midwife was with me as much as I wanted | 4.80 ± .405 | 4.39 ± .682 | −3.15 | .002* |
| The midwife gave me the care I needed | 4.82 ± .387 | 4.48 ± .658 | −2.90 | .004* |
| The midwife paid attention to my comfort during labour | 4.69 ± .557 | 4.50 ± .506 | −2.04 | .041* |
| The midwife communicated well with me | 4.82 ± .387 | 4.37 ± .610 | −3.87 | .000* |
| I'm satisfied with the privacy provided to me | 4.84 ± .367 | 4.48 ± .623 | −3.31 | .001* |
| Overall satisfaction | 4.78 ± .471 | 4.24 ± .603 | −4.60 | .000* |
*Mann–Whitney U test, significance level at p ≤ 0.05.
Table 4: Comparison of Mean Satisfaction between the Intervention and Control Groups
4.1 Interpretations of main findings
The mean pain scores of the intervention group were significantly lower than the control group at all measured points showing that application of single-use hot packs to the lower back in active phase of labour was effective in reducing labour pain intensity. The findings echo that of a study that reported significantly lower pain in women who received warm compresses compared to routine care18. Our findings are also consistent with reports that heat effectively decrease labour pain [19,20,21,22,27,34,35].
Findings of a clinical trial study shows that heat applied to lower back in the first stage and to the perineum in the second stage was effective in pain relief34. Another randomised control trial also reported a significant decrease in pain intensity among nulliparous women at 60, 90, and 120 min after the application of heat, to the sacrum–perineum in the active phase of labour [27]. It is note-worthy that the design and the site of application were not similar to our methodology. Further, cervical dilatation when pain was assessed also varied. Our participants were selected at 6–8 cm of cervical dilatation based on the hospital protocol as opposed to participants in other studies who were selected at 3–4 cm of cervical dilatation [35], 4–5 cm18, 5–6 cm20, 7 and 10 cm19. Our study participants had hot packs for a lesser duration that those in the other studies and no statistical difference was found in the duration of labour between the two groups. Overall, women in the intervention group had significantly higher satisfaction with their labour and delivery experience compared to the control group who also received intermittent Entonox inhalation as part of the routine care and could not be withheld for ethical reasons. Although, it is believed to increase the activity of inhibitory pain pathways in the brain, its role in pain relief remains unclear9. A Cochrane review of 26 randomised controlled trials in 2959 women showed that flurane derivatives were slightly more effective than nitrous oxide, although nitrous oxide helped to relieve pain when compared with no treatment [10]. In a comparison with oxygen, nitrous oxide found to be effective in labour pain relief [11]. We did not observe the amount, duration, and frequency of Entonox inhalation which may have influenced the findings. Despite the use of Entonox in the control group, heat application was found to be effective in relieving pain in the intervention group.
Contrary to our expectations, hot packs were not effective in reducing the duration of labour. Our results reinforce the findings of an experimental study that found heat was ineffective in reducing labour duration as compared with routine care18. However, conflicting results exist on its effect in different stages of labour. For instance, a randomised control trial found no difference in the duration of the first stage of labour between the warm pack group and the use of routine care and a birth ball [26]. Likewise, a randomised clinical trial reported no difference in the duration of the first stage labour [21]. Contrary to our findings, those authors reported a shorter third stage, which may be attributed to heat application on the perineum in the second stage. In a similar study, researchers used warm compresses in the first stage and heat to the perineum in the second stage and found no effect in the first stage but a significantly shorter second stage of labour [19]. Whereas another researchers reported a significantly shorter first and third stage of labour with the application of warm bags to the lower back in the active phase and to the perineum in the second stage [35].
Furthermore, researchers experimented with hot water bottles on the lower back and abdomen in the first stage and perineum in the second stage and reported shorter first and second stages of labour [20]. The heterogeneity in results can be attributed to variations in the study design. Unlike our study that used single-use instant hot packs at 30-minute intervals, with a rest period of 10 min, from 6–8 cm of cervical dilatation until delivery, heat was applied to the perineum in the second stage by other researchers, leading to conflicting results. Future studies can apply single-use hot packs on the perineum in the second stage of labour and test the effect on labour duration. Heat causes connective tissue elasticity, and the temperature level and duration of application may influence the effect of heat therapy on blood flow, tissue metabolism, and tissue elasticity [36]. Further, the use of Entonox by the control group may be attributed to the negative results on duration of labour, in our study. It’s role on uterine contractility is debatable. Entonox does not have an effect on uterine contractions or labour progression, however others claim its effectiveness in shortening the duration of labour [37]. For example, studies reported shorter first and second stages of labour and pain duration in women who received Entonox as compared to oxygen inhalation [10,11]. Researchers should consider this potential bias when designing future studies.
Women who received hot pack had significantly higher overall satisfaction with their labour and delivery experience as compared with those who received routine care. Our findings are comparable with findings of a randomised control trial who demonstrated the efficacy of heat in satisfying women in labour when compared to routine care [27]. Further, an experimental study reported moderate satisfaction with heat therapy18. Researchers recommended the routine provision of a warm shower for labouring women, reinforcing that it helped enhance their feeling of acceptance, making childbirth experience more positive as compared with the standard care group [22]. Heat in combination with other modalities has also shown to be satisfying to women in labour. High satisfaction was reported by those who had intermittent heat- and cold-pack application for pain relief during labour, whereas most women who received routine care reported low satisfaction [16]. Studies measured overall satisfaction using rudimentary scales such as the VAS & rating scale that do not identify individual aspects of satisfaction [18,27]. In that context, the strength of our study is that we used a 13-item valid and reliable satisfaction scale that measures various aspects of satisfaction.
4.2 Blinding
Blinding was not possible due to the nature of the intervention; the researcher’s presence may have positively influenced pain relief and satisfaction in the intervention group, causing a potential bias [27]. Two items, “because the midwife was with her most of the time” and “communicated and provided sufficient information and respected the women.” Were rated high on the satisfaction scale. It appears that the researcher’s presence and interaction might have enhanced satisfaction via facilitating women-centered care, which is one of the core concepts of midwifery care [22]. The researcher’s interaction may have been perceived as supportive, and the relief of pain, comforting. Contentment is due not only to the pain relief but also the care provided38. According to Kolcaba (1990), specific interventions enhance comfort through a sense of relief, ease, and transcendence [39]. It may be noted that two items, “I was happy about the care I received” and “I was happy about the labour and delivery experience,” were not significantly different between the two groups. It is possible that the word satisfaction would have been more appropriate in place of happy in these two items. A factor analysis would provide information on the factor structure of the LDSS.
The control group, who received self-administered Entonox inhalation, had lower satisfaction levels than that of the intervention group. It is possible that, like most nonpharmacologic pain management methods, hot pack, which is effective in reducing pain intensity, has no side effects and has the potential to promote control, thereby achieving a positive birth experience. We did not assess the self-control of the women during labour. However, future studies can incorporate self-control as a variable and its relationship with pain and satisfaction.
4.3 Limitations
Although the strength of this study is that it is the first to determine the effect of single-use hot packs on pain and duration of labour with an adequate representative sample, some potential limitations should be considered when interpreting the results. First, due to the labour room protocol, our participants were selected at ³6 cm cervical dilatation, thereby restricting the generalizability of the findings to only those with ³6 cm of cervical dilatation. Second, the control group had the choice of intermittent self-administered Entonox as part of routine care. We did not observe the duration and amount of its use which might influence the validity of the findings. Third, the nature of the intervention rendered blinding impossible, thereby introducing an element of bias. Fourth, data on cervical dilatation was calculated from the patient records which may have affected the validity of the findings. Fifth, although the validity and reliability of the LDSS is established, a factor analysis would help establish the instrument’s construct validity. 1.Conclusion
The study provides evidence that application of single-use hot pack in active phase of labour can effectively reduce labour pain intensity; however, is not effective in reducing duration of labour. This non-pharmacological method is a promising option for pain relief because of its ease of application and does not need training of the nurses/midwives. It, however, requires them and the women to ensure measures to avoid burns at the site of application. Continuing education for nurse/midwives should emphasize heat therapy as a non-pharmacological measure for pain relief in labour. Nurse administrators must encourage the use of hot packs in labour room settings, to provide a satisfying labour and delivery experience to the women in labour. It would be prudent to conduct future studies where Entonox inhalation is not a part of routine care.
Funding: declared
Data availability statement
Datasets related to this article can be found in an open-source online data repository hosted at Mendeley Data: XXXXX “Effectiveness of Hot Pack on Labor Pain, Duration of Labor, and Satisfaction of Primigravida: A Randomized Controlled Trial”, Mendeley Data, XXXXXX
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti
