AUCTORES
Globalize your Research

Research article | DOI: https://doi.org/10.31579/2641-0419/234
1Cardiothoracic Centre, All India Institute of Medical Sciences, New Delhi, India.
2Department of Cardiothoracic Surgery, All India Institute of Medical Sciences, Himachal Pradesh, India.
*Corresponding Author: Ujjwal Kumar Chowdhury, MCh, Diplomate NB ProfessorDepartment of Cardiothoracic and Vascular Surgery All India Institute of Medical Sciences Ansari Nagar, New Delhi-110029, INDIA.
Citation: Shikha Goja, Lakshmi Kumari Sankhyan, Ujjwal K. Chowdhury, Niraj N. Pandey., Sudheer Arava., et all (2022). Echocardiographic and Computed-tomographic Evaluation of the Fate of Bovine Pericardial Patch as a Pericardial Substitute in Bentall’s Procedure: Twenty-year’ Results. J. Clinical Cardiology and Cardiovascular Interventions, 5(1); DOI:10.31579/2641-0419/234
Copyright: © 2022 Ujjwal Kumar Chowdhury, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November 2021 | Accepted: 30 December 2021 | Published: 06 January 2022
Keywords: annuloaortic ectasia; aortic dissection; bentall’s procedure; bovine pericardial patch; pericardial calcification
Objective: The study was designed to ascertain the influence of usage of bovine pericardial patch in patients undergoing Bentall’s procedure with respect to reexploration for bleeding, mediastinal infection, avoidance of conduit adhesions, late development of pericardial constriction and calcification.
Materials and Methods: We reviewed 150 patients (79 males) aged between 22 to 68 years (mean±SD 49.25±12.9 years) receiving a composite aortic conduit between January 1998 to December 2020 for annuloaortic ectasia (n=100), aortic dissection (n=49), and dilated aortic root in repaired tetralogy of Fallot (n=1). Twenty-five patients had Marfan’s syndrome. Modified “button technique” was performed by interposing a glutaraldehyde treated pericardial strip at the graft coronary anastomoses, and proximal aortic conduit suturing using interlocking interrupted, pledgeted mattress suture. On completion, the pericardial cavity was reconstructed using St. Jude Medical Biocor pericardial patch. To detect evidence of pericardial constriction, survivors underwent echocardiography and computed tomography. The Kaplan-Meier curve was drawn to show the probability of survival over a period of follow-up time.
Results: Seven (4.7%) patients died of cardiac-related cause, 45% had transient hemodynamic instability, 55% had low cardiac output, and 87.1% had spontaneous return of sinus rhythm. The average 12-hour postoperative drainage was 245±70 ml and there was no mediastinal infection. At a mean follow-up of 172.4 (SD± 58.9) months, the actuarial survival was 94.2±0.04% (95% CI: 88.5-96.8), and there was no pericardial constriction or calcification.
Conclusion: Reconstruction of pericardial cavity using Biocor bovine pericardial patch minimizes diffuse oozing of blood, graft infection, and is not associated with later development of pericardial constriction, or calcification.
Since the introduction of glutaraldehyde by Alain Carpentier, bovine pericardium and other biological tissues have been used in clinical practice for the past 50 years. The biological tissues when subjected to low concentration of glutaraldehyde loses its antigenicity, does not induce the formation of antibodies, and produces the disruption of intra- and intermolecular protein, enhancing its structural stability, and maintaining sterility. [1-4]
The glutaraldehyde-treated bovine pericardium is one of the biological materials widely used in cardiovascular surgery as a patch material for aorta, pulmonary arteries, medium sized vessels, bioprosthesis valve leaflets, for repair of intracardiac defects, small vascular substitutes, and neoaortic reconstruction. The non-cardiac usage has been during tracheal reconstructive surgery, repair of diaphragmatic defects, and suture line reinforcement during lung volume reduction procedures, cholangioplasty, and inguinal hernia repair. [2,3,5-21]
Literature documents isolated case reports on successful use of bovine pericardium in infected surgical field, namely, patch arterioplasty, and patch reconstruction of the mitral annulus following infective endocarditis.[22] However, larger case series as well as long-term results of use of this biomaterial in presence of infection is not available.[13,21,23-28]
The original Bentall’s procedure employed an in situ circumferential suture line around the coronary ostia, then complete aortic wrap around to control bleeding. Tension developing at the suture line of the side-to-side coronary anastomosis and/or blood accumulation within the perigraft space conveyed significant risk of coronary artery dehiscence, pseudoaneurysm formation and reoperation.[29,30] Hematoma in the space may additionally compress the graft or cause prosthetic valve dysfunction.[31-33]
To avoid this complication, Cabrol used a fistula to the right atrial appendage and subsequently adopted interposition Dacron conduits to the coronary ostia with the new risk of graft thrombosis and persistent aorto-right atrial fistula.32 For these reasons, a modified open technique was developed by Kouchoukos and associates in 1986 that eliminated the prosthetic wrap and allowed reattachment of adequately mobilized coronary buttons to the graft with tension free sutures. [29]
Despite technical improvements in coronary arterial reconstruction by the “open button technique”, graft-coronary anastomotic bleeding, bleeding from proximal and distal aortic conduit suture line, pseudoaneurysms of the coronary ostia anastomoses, pseudoaneurysms of the proximal and distal suture lines continue to occur because of fragility and reduced tissue quality of the ascending aortic wall and connective tissue abnormality. [20,31,34-41]
To address these concerns, we interposed a glutaraldehyde-treated autologous pericardial strip between the graft and native coronary ostia during coronary ostial implantation and placed interlocking, interrupted, pledgeted mattress sutures to ensure perfect hemostatic proximal aortic suture lines. The technical details and long-term results of coronary ostial and distal aortic anastomoses following modified Bentall’s procedure have been addressed in our previous publications. [42-46]
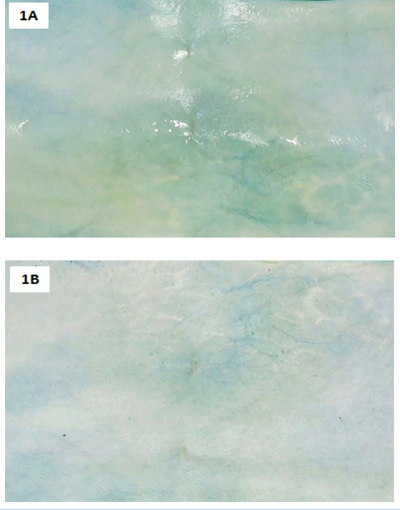
Since the native pericardium was harvested for creating coronary buttons, bovine pericardium was used to cover the cardiac chambers and great vessels, including the conduit. From 1998 onwards, we reconstructed the pericardial cavity using a bovine pericardial patch to reduce/eliminate diffuse oozing from multiple needle holes and graft interstices, prevent the formation of postsurgical adhesions between the conduit and sternum, and as a protective material against graft inoculation (Figures 1A, 1B).
Bovine pericardium is preferred because it’s biocompatible, less antigenic, resistant to infection and acellular comprising essentially of pure collagen which may provide a natural microenvironment for host cell migration and proliferation, accelerating endothelization and tissue regeneration. [5-21]
Bovine pericardium is thoroughly washed and sutured with the rough surface facing intrapericardial side. Experimental data have demonstrated formation of covering layers with more plasticity, producing greater tension resistance and expansion when the rough face was placed intraluminally towards the vessel lumen, thus preventing aneurysmal dilation. [47]
The technical details of coronary button implantation, the long-term fate of coronary ostial and distal aortic anastomoses, and the myocardial preservation strategies of this group of patients have already been addressed in our previous publications. The same is not repeated here. [42-46] In this retrospective study, we present the very late-term (20 years) results evaluating: i) any reduction of diffuse bleeding and perioperative prosthetic graft infection, ii) the stability of newly reconstructed pericardial cavity over time, and iii) the fate of bovine pericardial patch in terms of thickening, constriction, and calcification assessed using echocardiography and computed tomography.
This study conforms to the principles outlined in the declaration of Helsinki of 1975, as revised in 2008. Between January 1998 to June 2021, 150 consecutive patients (79 males), aged 22-68 years (mean 49.25±12.9 years) underwent modified Bentall’s operation using the surgical techniques described after obtaining informed consent and institutional ethics committee approval. This is the total number of Bentall’s procedure done by the corresponding author in the last 23 years, and all patients are included in this study. Literature does not document any other studies citing the use of bovine pericardium as a pericardial substitute in patients undergoing Bentall’s procedure. Therefore, the total number of operated patients in this study is totally based on subjective assessment by the corresponding author. Indication for surgery included annuloaortic ectasia (n=100), type A aortic dissection (n=49) and dilated aortic root following intracardiac repair of tetralogy of Fallot (n=1). Moderate to severe aortic regurgitation was seen in 144 (96%) patients, 6 (4%) patients had grade II mitral regurgitation, and 105 (70%) patients had left ventricular ejection fraction <0>Table 1.
Echocardiography
Transthoracic two-dimensional, color-flow Doppler echocardiography (Philips iE33 echo machine; Philips X7-2T probe, Bothell, WA, USA) was performed to measure mitral, tricuspid, superior vena cava, hepatic vein, pulmonary venous flow velocities, prosthetic valve motion, and transprosthetic gradients. Mitral or tricuspid regurgitation was assessed semiquantitatively as grade 1+ to 4+. Ejection fraction was calculated with a modification of the method of Quinones and colleagues. [48] A constrictive pattern was defined as pericardial thickening >4mm, 25% or greater increase in mitral E-velocity with respiration, and an augmented (25% or more) diastolic flow reversal in the hepatic vein after the onset of expiration compared with the inspiration phase.[49,50]
Techniques of computed tomography
Non contrast high pitch spiral acquisition was performed using a dual source computed tomography scanner (Somatom flash/ force, Siemens Healthcare, Forchheim, Germany). The scan was acquired in a craniocaudal direction, from above the level of carina upto the diaphragm.
Thin axial sections (1.0 mm, increment 0.6 mm) were reconstructed using a medium-soft convolution kernel (B26). All reconstructed images were transferred to an external dedicated workstation (syngo.via, Siemens Healthcare, Forchheim, Germany) where multiplanar reformations, and volume rendered images were evaluated alongside axial images.
Surgical techniques
Intraoperative transesophageal echocardiography was performed with a Hewlett-Packard Sonos 1500 or 5500 ultrasound system on all patients. Standard anaesthetic and operative techniques were used throughout the study period. The operations were performed under moderately hypothermic cardiopulmonary bypass through arterial cannulation (axillary artery n=28; femoral artery n=122) and bicaval venous cannulation of femoral vein and superior caval vein.
A retrograde coronary sinus cannulation with self-inflatable balloon (RCO 14, Edwards Lifesciences, Irvine, CA, USA) was done using transatrial blind cannulation in 100 patients. In cases of difficult cannulation (n=50), the coronary sinus was cannulated through a short right atriotomy under direct vision. Proper placement was confirmed by observing distension of posterior interventricular vein, maintenance of coronary sinus pressure, palpation of coronary sinus cannula posteriorly at the base of heart and transesophageal echocardiography.[51] No coronary sinus anomalies or coronary sinus injuries were confronted.
Ultrafiltration was used in all patients during and after cardiopulmonary bypass to reduce the total body water, potassium overload and to remove the inflammatory mediators from the circulation, maintaining hematocrit more than 25% on cardiopulmonary bypass.
All patients were subjected to the “integrated myocardial preservation management” strategy using intermittent antegrade direct ostial cardioplegia and retrograde coronary sinus cardioplegia infusion.[52] Cardioplegic infusions by both routes were never given simultaneously.
A dacron composite graft with a mechanical heart valve [(St. Jude Medical Inc.; Minn); (Conduit 25 mm (n=60); 27 mm (n=55); 29 mm (n=35)) was used in all patients. While creating the coronary buttons, the pericoronary diseased aortic tissue was excised leaving behind a cuff of 10-12 mm.
All patients in the study underwent “modified button technique” for reconstruction of the coronary arteries and proximal conduit suturing for perfect hemostasis (Figures 2A-2I).
The technical details of the composite aortic graft replacement, the fate of the coronary ostial, and distal aortic anastomoses, and the myocardial preservation strategies have been enumerated in detail in our previous publications.42-46 The composite graft was sutured to the annulus using everted, interrupted 2-0 sutures over polytetrafluoro-ethylene pledgets. Each interrupted aortic supra-annular sutures were placed in such a fashion that successive sutures were made to pass through the previous pledget; thus ensuring perfect aortic annular hemostasis (Figures 2A, 2B). Using graft cautery, two side holes were created on the composite graft measuring around 10mm in diameter in the proposed area of coronary ostial implantation. The left and right coronary buttons were anastomosed in an end-to- side fashion with continuous 5-0 polypropylene suture to openings on the composite graft. While suturing, a long strip of glutaraldehyde treated pericardium, about 1 cm wide was interposed circumferentially around each graft-coronary button anastomosis (Figures 2C-2H). During construction of the inferior portion of the ostial anastomoses, the continuous retrograde perfusion was transiently lowered to avoid flooding and performing perfect hemostatic suturing under vision.
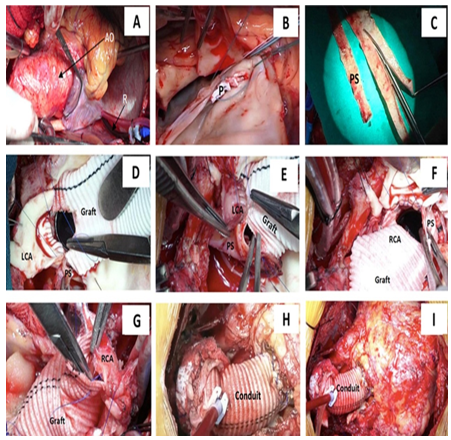
The right coronary button was anastomosed at a relatively high position of the composite graft taking into consideration the collapsed state of the right ventricle during cardioplegic arrest. We used topical thrombin (Tisseel, Baxter AG, Vienna) as an additional topical hemostatic agent on all patients.
Mean cross-clamp time was 114.6±28.4 min (range, 90-187 minutes) and mean cardiopulmonary bypass time was 156.0±29.6 min (range, 136-220 min).
Following removal of aortic cross-clamp, majority of the patients (n=132, 87.2%) returned to normal sinus rhythm. Only 18 (12.8%) patients required antegrade administration of injection adenosine and 200-250ml warm hotshot blood cardioplegia for spontaneous defibrillation. Direct current cardioversion was not used on any patient. We used atrioventricular sequential pacing for 24-48 hours in patients with low heart rate.
On completion of the Bentall’s procedure a segment (15 x 10 cm) of bovine pericardium (SJM BiocorTM Pericardial Patch, St. Jude Medical, St. Paul, MN, USA) was used to cover the cardiac chambers and great vessels including the valve conduit (Figures 1A, 1B).
Statistical Analysis
Statistical analysis was performed using Intercooled STATA 14.0 Software (College Station, Texas, USA). Interval related data were expressed as mean ± standard deviation (SD) or median (minimum-maximum) and categorical variables were expressed as percentages. The Kaplan-Meier curve was drawn to show the probability of survival over a period of follow-up time. The results were expressed as probability of survival (95% confidence interval) at various time intervals. Statistical significance was set at p<0>
Short-term outcomes
There were 7 (4.7%) early deaths due to low cardiac output syndrome with multiorgan failure and superimposed sepsis between 10th to 18th postoperative days. These patients had acute type A aortic dissection and were in congestive cardiac failure preoperatively (Table 1).

Patients who needed moderate amount of inotropes (usually dopamine and/or dobutamine hydrochloride, 5 µg/kg/min) for less than 24 hours postoperatively were considered as having transient postbypass hemodynamic instability (n=72). In contrast, patients who required inotropic agents, vasopressors and/or intra-aortic balloon counterpulsation for more than 24 hours postoperatively were categorized as having a true low cardiac output syndrome (n=78).
Five patients required intraoartic balloon counterpulsation as an additional support of which three patients survived. The incidence of low cardiac output syndrome remained fairly constant over the course of the study.
Morbidity
Hospital morbidity included re-exploration for excessive bleeding from non-anastomotic sites within 12 hours in 8 patients with acute type A aortic dissection. The average 12-hour postoperative drainage was 245±70 ml. Twelve (9.2%) patients required tracheostomy and long-term ventilator support. Hospital stay ranged from 7 to 54 days (median, 9 days; mean, 20±7 days). Three patients were readmitted on 18th, 21st and 22nd days postoperatively had deranged prothrombin time and required pericardiocentesis.
Long-term outcomes
There were 3 (2%) late deaths at 15 and 69 months after surgery due to intractable ventricular arrhythmias and anticoagulant-related intracranial bleed respectively. Follow-up was 100% complete (1-226 months) and yielded 1218 patient-years of data. At a mean follow-up of 172.4 (sd± 58.9) months, the actuarial survival was 94.2±0.04% (95% CI: 88.5-96.8). All survivors were in New York Heart Association I or II at their last follow-up. Two patients required thoraco-abdominal aortic graft replacement with re-implantation of celiac, superior mesenteric and right renal arteries 3 years following Bentall’s procedure. No survivors had structural deteriorations, pseudoaneurysm formations or thromboembolic complications.
Peri-operative myocardial infarction and arrhythmias
No patients sustained a perioperative myocardial infarction. Postoperatively, 16 (10.7%) patients had supraventricular arrhythmias, 8 (5.4%) had premature ventricular contraction, 2 (1.3%) had ventricular tachycardia, 14 (9.3%) had left bundle branch block, and 10 (6.7%) had junctional rhythm. No patient had complete heart block.
Postoperative studies and results
Cohort of survivors
All survivors (n=140) were examined and studied between December 2019 and June 2021, which was the closing interval of the study. Postoperative evaluation consisted of clinical examination, electrocardiogram, chest radiograph, cine fluoroscopy, echocardiography and computed-tomographic angiography. The functional class at follow-up was noted. All patients received warfarin and aspirin (100 mg/day) for anticoagulation to maintain INR between 2.5 to 3.5. Digoxin and diuretics were weaned at varying time intervals. Amiodarone was used for intractable atrial fibrillation.
Postoperatively, the left ventricular ejection fraction increased from 50%±9.2% (range 15% to 62%) to 58%±6.2% (range 15%-70%). Thirty-nine (26%) patients had left ventricular ejection fraction ranging between 15% and 25%.
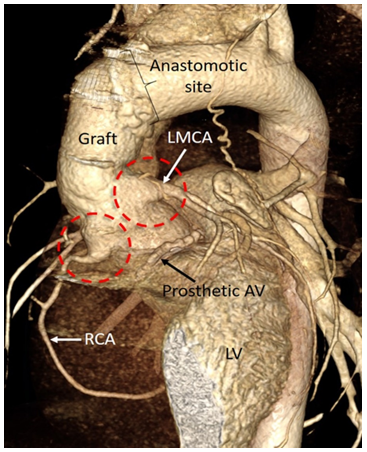
At a mean follow-up of 172.4±58.9 months, none of the survivors demonstrated anastomotic complications involving the coronary ostia or the distal aortic arch. All patients demonstrated patent coronary ostia and with no coronary aneurysm, kinking or pseudoaneurysm formation of the newly implanted coronary arteries (Figure 3). None of the survivors had either constrictive pericarditis or pericardial calcification.
The present study is the first to our knowledge to determine the very late-term (20 years) results of bovine pericardium as a pericardial substitute in the setting of Bentall’s operation. The study provided several interesting findings: i) no patient exhibited clinical or echocardiographic features of constrictive pericarditis, ii) computed-tomography did not reveal any instances of pericardial thickening or calcification and iii) the average postoperative drainage volume was 249±65 ml in the first 12 hours following surgery, with no instance of graft/mediastinal infection on any patient.
The quest to establish a pericardial substitute that is durable for 20-25 years without causing any pericardial adhesions, and adverse hemodynamics continues. Various biologic or synthetic sheets such as absorbable polymer patches, three-layered synthetic pericardial substitutes, and expanded polytetrafluoroethylene have been used as a pericardial substitute.[52-54] However, there have been no documented adequate substitutes that reduces postsurgical adhesions.[53] Prevention of adhesions through pericardial substitution has therefore become a matter of investigation.[55]
Bovine pericardium has come into common clinical use during the past 50 years, especially when used as a patch for arterial closure during vascular and cardiac surgery. Technical merits that have led to widespread adoption of bovine pericardial patches in the operating room, include easy handling, less suture bleeding and the ability to immediately perform arterial duplex examination at the site of angioplasty.[5-21] However, long-term results of this biomaterial are poorly documented and need cautious interpretation as to whether its long-term performance is related to the material itself or to the operation in which it is used.[1,13,14]
Experimental basis and clinical applications of bovine pericardium as a biomaterial
The advantages of bovine pericardium as a cardiovascular patch can be divided into clearly observed and documented advantages, and benefits that are not well documented so far. The clearly documented advantages are: i) biocompatibility; ii) minimized antigenicity, increased strength and stability due to pretreatment using glutaraldehyde; iii) dependable suture retention due to consistent processing with 0.5 mm thickness pericardium; iv) reduced potential infections; v) increased long-term durability; vi) similarity of compliance of bovine pericardium and native artery/prosthetic conduit; and vii) feasibility of insonation with ultrasound immediately after implantation due to lack of air spaces and solidity.[3,21,25,26,57-59]
Although being used in clinical practice, there are instances where benefits of bovine pericardium not as well documented, for example: i) use of bovine pericardium as a vascular patch of medium sized arteries namely, carotid, femoral, and popliteal arteries following embolectomy or endarterectomy, ii) closure of intracardiac defects like atrial and ventricular septal defects,[5,7,17] iii) repair of arteriotomy in the presence of infected field despite lack of evidence of it being bacteriostatic or bactericidal,11,12 and iv) claim of some manufacturers that bovine pericardium possess anticalcification technology that can significantly reduce calcification, and support endothelization.[8,9,27,6-65]
Bovine pericardium being an acellular material of essentially pure collagen, may provide a natural microenvironment for host cell migration, and proliferation, accelerating endothelization, and tissue regeneration.[66,67] Since primary closure of a longitudinal arteriotomy may result in restenosis due to neointimal hyperplasia, patch arterioplasty is advocated to prevent this complication. Most commonly, patch angioplasty is performed after carotid endarterectomy and in femoral and popliteal arteries following thrombectomy or embolectomy. Meta-analysis provides strong evidence that carotid patching provides both perioperative and long-term benefits after carotid endarterectomy.[8,9,11,27,61-63,65,68-74]
Published literature is divided on the selection of patch material for carotid endarterectomy. Vein patch angioplasty ideally should have the lowest incidence of postoperative thrombosis due to an intact endothelium, an inherent suppleness and natural compliance. Several investigators have reported equally encouraging results using bovine pericardial patch and synthetic patches.[61,69-72]
Although there are morphological similarities, the molecular and cellular pathways that stimulate intimal hyperplasia in these clinical circumstances may be different. The biological signaling pathways that activate vascular healing after patch angioplasty depend on cells that infiltrate the patch and different patches may have different biological responses and therefore may need different types of treatment.[8,9,11,27,61-63,65,68-74]
Although scientific evidence of bovine pericardium as bacteriostatic and bacteriocidal is scanty, it has been used to repair arteriotomy in the presence of infected field.[11-14,21,25-27,74,75] Prosthetic patch infection after carotid endarterectomy has been estimated to be around 0.4%.26,75 Investigators have demonstrated similar risk of postoperative infection comparing bovine pericardium, autologous vein patches, and synthetic patches.[6,11,12,74,75] However, until an underlying mechanism of resistance to infection e.g. contact cytotoxicity is demonstrated, one cannot convincingly state that bovine pericardium is immune from becoming infected. The fundamental strength of glutaraldehyde fixed bovine pericardial patch may be responsible for low rate of degeneration and resistance to infection.
Fibrosis of patches is unusual and reports of bovine pericardium patch fibrosis are distinctly rare.[77,78]. It is likely that the mechanisms that induce patch calcification may be similar to those that induce patch fibrosis, although with subtle differences. Further research may help identify fibrocyte-specific signaling pathways as potential therapeutic targets to prevent bovine pericardium fibrosis.[79]
Since the primary problem of xenografts is structural deterioration at long-term, mainly due to calcification, several improvments in the processing of xenografts and placement of the pericardial patches have been implemented to prevent structural deterioration and dystrophic calcification.[8,9,46,80-83]
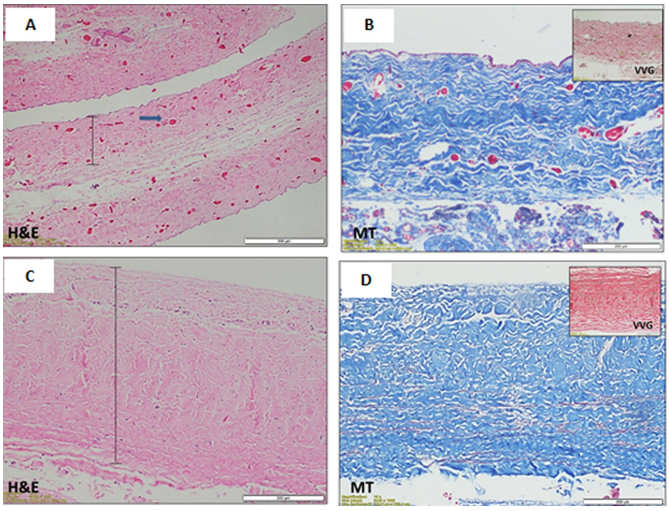
The native structure of bovine pericardium has three layers: i) the thin inner serosal layer consisting of mesothelial cells; ii) the thicker fibrosal layer formed by diversely oriented, wavy bundles of collagen and elastin; and iii) the outer epipericardial connective tissue layer that is partly continuous with the pericardiosternal ligaments (Figure 4A-4D).
Commercially available patches are processed to be acellular, preventing transplantation of bovine proteins or DNA into the host. Gluteraldehyde is a typical processing agent, crosslinking −NH2 groups of lysine, hydroxylysine, or the N-terminus of amino acids, to form amine linkages with the elimination of water; these amine linkages form covalent bonds between adjacent proteins that are stable at physiological temperature and pH. The resultant cross-linkage of xenograft tissue with glutaraldehyde increases tissue strength to inhibit biodegradation, stabilizes collagen, and reduces antigenicity.[1,57,66,67,80-92]
However, glutaraldehyde fixation promotes dystrophic calcification because of the chemical process between free aldehyde groups, phospholipids, and residual antigenicity of the bioprosthetic tissue.[1,80-85] Series of experimentation over several years through basic research have been directed toward developing a tissue treatment process to prevent calcification in glutaraldehyde fixed xenograft tissue. The aim of the anticalcification strategies is to extract lipid or to neutralize toxic residual aldehyde.[92-95]
Residual free aldehyde groups or polymerized forms of glutaraldehyde create a locally cytotoxic environment and result in tissue calcification. Amino acid post fixation improves protein cross-linking to increase the mechanical performance of bioprostheses or to neutralize these free aldehyde groups because the amino groups of these compounds can react with the free aldehyde groups of glutaraldehyde, forming Schiff base.[86,87,94,95] In 2009, Zhou et al demonstrated utiliy of sodium bisulfite, a classic reductive agent which reacts with aldehyde to form -hydroxyl sodium sulfonate, and would react with any free glutaraldehyde in fixed pericardial tissue, thus minimizing in vivo calcification.[96]
Short-chain alcohols, such as octanol at high concentration (>50% in aquous buffers) reduce calcification potential of aldehyde-fixed tissues by removing phospholipids or conformational changes in collagen.[87,92,93] The alcohols may also be preferentially bound to hydrophobic residues within collagen and elastin which may undergo independent calcification.[88,97]
Long-chain alcohols such as oetanol 1, 2-octanediol along with short-chains, and isopropanalol have been used along with a buffered ethanol solution to remove phospholipids more efficiently.[90,92,93,98]
The key common feature for the pathophysiology of calcification is involvement of devitalized cells and cellular debris.[80-83] There is a debate in the literature as to whether there is an immune response to bioprosthetic tissue.[80-83] Recently, it has been found that the mammal cell surface xenoantigen called -Gal epitopes are still present on the commercially available glutaraldehyde fixed tissues.[84] Patients undergoing bioprosthetic valve implantation have exhibited a significant rise in anti--Gal antibodies.[99-104] Decellularization suppresses the rise anti--Gal antibodies titre. However, the pathogenesis of dystrophic pericardial calcification remains conjectural.
Other investigators have introduced genipin, derived from the fruits of Gardenia Jasminoides as a novel cross-linking agent because this naturally occurring cross-linker is less cytotoxic and better in vivo biocompatible than glutaraldehyde.[66,67,89] Park and associates have used recombinant human alpha galactosidase A to remove alpha-gal epitopes from porcine aortic valve.[105-107]
Despite good results of bovine pericardium in several clinical trials, degeneration of biological tissue including calcification is frequently observed.[80-83] Piers and colleagues suggested a possible correlation between calcification and contact of the rough face of the pericardium with the blood stream.[8,9] In 2011, Saporito and colleagues demonstrated experimentally that the bovine pericardium preserved in glutaraldehyde did not show alterations in its structure when implanted with different faces turned to the inner portion of vessels.[46] There was aneurysmal dilation of the implant site when the smooth face was turned to the intraluminal side. When the rough face was turned intraluminally, there was formation of a covering layer with more plasticity, modeling elastic tendon and bone formation which produced greater tension resistance, preventing its expansion. Piers and colleagues demonstrated the formation of internal apposition fibrosis on the surface of the retail. The wrinkled surface of the retail facilitates capture and adhesion of blood components and subsequent assemblage by the release of platelet factors and secondary released thromboplastin.[8,9,108] In this study, all patients underwent reconstruction of the pericardial cavity using bovine pericardium with the rough surface facing the cardiac chambers, and great vessels.
Some investigators have reported that if smooth muscle cells and/or fibroblasts migrate into the bovine pericardium patch, the patch may provide an environment that promotes subsequent calcification and degradation.[94,95] Hruska and associates summarized the currently accepted major theories regarding the mechanism and regulation of vascular calcification: i) abnormal calcium and phosphate homeostasis, ii) failure of anticalcific mediators, iii) induction of osteochondrogenesis, iv) apoptosis, v) circulating nucleatic complexes/paracrine factors derived from bone, and vi) matrix degradation.[109-113]
As these etiologies become more understood, it is possible that preventive strategies may be able to be incorporated into future generations of patches, i.e. incorporation of anticalcific mediators, remesothelialization on the surfaces of the implanted patch. [97,98,101-104,109-113,119,120] These next generation patches might be particularly useful for patients with chronic kidney disease, type 2 diabetes mellitus, and elderly, who might be at increased risk of patch calcification and degradation.[114]
When bovine pericardium is used as a vascular patch, the collagen surface of the bovine pericardial patch may be a nidus of thrombus formation. However, thrombosis of bovine pericardium patches has not been reported to be a major problem, either acutely or chronically. In clinical practice, most institutions routinely administer Dextran-40 for 24 hours post endarterectomy to prevent thrombus formation and propogation at the site of thromboendarterectomy.
Exploring the unknown: Future Directions
This communication is not meant in any way to convince those surgeons satisfied with their own methods of performing a Bentall’s procedure. Rather it hopes to pointout that reconstructed pericardial cavity is beneficial preventing inoculation with infected mediastinal wound, minimizes diffuse oozing, and avoids postsurgical periconduit adhesions.
Can intimal hyperplasia be avoided by seeding mesenchymal stromal cells on bovine pericardium? Investigators have used bovine pericardium as the scaffold for the seeded multilayered mesenchymal stromal cells to provide a base for uniform cardiac tissue regeneration.115 They have demonstrated that this novel bioengineered tissue graft can serve as a useful cardiac patch to restore the dilated ventricle and stabilize cardiac functions after myocardial infarction.115 Interestingly, the authors reported increased density of neomicrovessels in the tissue engineered patches compared to control patches, suggesting that tissue regeneration occurs within the porous bovine pericardium through a process involving cell recruitment and tissue-specific differentiation.
Investigators have demonstrated that acellular bovine pericardial tissues fixed with genipin could provide a natural microenvironment for host cell migration, and may be used as a tissue engineering extracellular matrix to accelerate tissue regeneration.115 In an attempt to reduce postsurgical pericardial adhesions, researchers are experimenting on mesothelial regeneration on acellular bovine pericardia loaded with an angiogenic agent (ginsenoside Rg1).[66,67,105-107,115-120] This exciting research shows the prospect for delivering cell therapy, in a site-specific manner, with bovine pericardial patches.
Conclusions
Reconstruction of the pericardial cavity using bovine pericardial patch minimizes diffuse oozing of blood, mediastinal infection, and is not associated with late development of pericardial constriction and calcification. Understanding the mechanisms by which bovine pericardium heals after patch angioplasty may lead to next generation tissue engineered patches. Process of decellularization, use of alcohol, newer preservatives like genipin and mechanism of healing of bovine pericardial patches may improve the long-term durability of bovine pericardial patch.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Giselle Pentón-Rol.
