
Research Article | DOI: https://doi.org/10.31579/2637-8892/336
Department of Psychology University of Nigeria, Nsukka, Nigeria.
*Corresponding Author: Emmanuel O. Ugwu, Department of Psychology University of Nigeria, Nsukka.
Citation: Immanuel U Euckie, Emmanuel O. Ugwu, Ikechukwu C. Eze, Chinwendu G. Ezea, Obinna M. Ezeora, et al, (2025), Brain Fag Syndrome – Neglected, But Revisited, Associated with Suicidal Ideation, and Moderated by Assertiveness, Psychology and Mental Health Care, 9(5): DOI:10.31579/2637-8892/336
Copyright: © 2025, Emmanuel O. Ugwu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 May 2025 | Accepted: 06 June 2025 | Published: 20 June 2025
Keywords: brain fag syndrome; suicide; assertiveness; psychopathology
Background: Brain Fag Syndrome is a disorder known since 19 century to affect the cognition of people. The few studies of Brain Fag Syndrome in literature described it as a culture bound syndrome; it was neglected without much research, yet it has been devastating the lives of people.
Aim: The present study revisited Brain Fag Syndrome, and investigated its associations with suicidal ideation and assertiveness.
Method: Two thousand, seven hundred and forty-five participants drawn from West Africa, were involved in this study. The authors employed the Brain Fag Syndrome Scale, Assertive Behavior Inventory, and Positive and Negative Suicidal Ideation – Negative Ideation Sub-Scale for data collection. The participants’ ages were 15 – 71 years. The authors used cross-sectional design, and PROCESS Macro for data analysis.
Result: The authors found that Brain Fag Syndrome positively associates with suicidal ideation, assertiveness negatively associates with suicidal ideation, and assertiveness moderates the relationship between Brain Fag Syndrome and Suicidal ideation.
Conclusion: Brain Fag Syndrome is a serious psychopathology that demands attention of the international community, as it engenders suicide. Self-expression, the hallmark of assertiveness has a way of mitigating the course of Brain Fag Syndrome so that it does not necessarily end in suicide.
Brain fag syndrome (BFS) is an expression of psychological distress that was first described in Nigeria by Raymond Prince (1960; 1962; 1979; 1983; 1985). BFS describes a set of symptoms including difficulty in concentrating and retaining information, head and neck pains, and eye pain (Ayonrinde, 2020; Katona & Robertson, 2005; Ola et al., 2009). BFS symptomatology include: somatic complaints (pains and burning sensations around the head and neck), cognitive impairments (inability to grasp the meaning of written and sometimes spoken words, poor concentration and retention), sleep-related complaints (fatigue and sleepiness in spite of adequate rest) and other somatic impairments, such as blurring, eye pain and excessive tears (Minde, 1974; Ola et al., 2009; Ola & Igbokwe, 2011). Brain fag syndrome has been identified in some other countries including Uganda (German & Arya, 1969; German & Assael, 1971; Minde, 1974), Liberia (Thebaund & Rigamer, 1976), Ivory Coast (Parin, 1984), and Malawi (Peltzer, 1987). BFS was regarded as a disorder of simple exhaustion of the nervous system resulting from active overwork (Richardson, 1870). It was seen as insanity, arising from excessive mental work (Tuke, 1880). Tuke called brain fag brainworkers disorder (Tuke, 1892). Brain-fag was symptomized with sensations of pressure in the head; poor memory, lack of concentration, irritability of temper, increased reflexes, poor sleep, anorexia and various aches and pains before 1960 (Gillespie, 1926). There was a clinical observation of bran fag from Guy’s Hospital, London with the following symptoms poor memory, excessive fatigue, irritability, or insomnia by Gillespie (Gillespie, 1933). In America, Mary Bayley related brain fag disorder to academic stress (Bayley, 1917). The BFS was captured in DSM IV TR as psychopathology characterized by certain anxiety, depressive and somatoform disorders specifically from West Africa with the term culture bound syndrome (APA, 2000). Argument and criticism over the term culture bound syndrome like “Why is it that the non-Western disorders are contextualized in non-Western cultures, but those identified and coded in the West in DSMs and ICDs are the real thing? Certainly, they are as much cultural products as are those from non-Western cultures (Marsella & Yamada, 2010). This criticism and other cultural debates made the newer versions of DSM-5 recognize BFS, but less detailed and not with the term “culture bound syndrome”. BFS was cited in DSM-5 as cultural anxiety syndrome. It was included into types that deal with cultural concepts of distress; cultural syndrome (clusters of symptoms that may be related to but need not be “bound” or limited to local cultures), idiom of distress (everyday ways of talking about distress that cut across syndromes) and causal explanation, DSM-5 (APA, 2013). The cluster of mental exhaustion symptoms is classified under the rubrics of depression, anxiety, somatoform and medically unexplained disorders in the prevailing World Health Organization and American Psychiatric Association classificatory systems including ICD 10 (Segal, 2010); ICD 11 (World Health Organization, 2019); ICD 10 (World Health Organization, 1992); DSM-IV-TR (APA, 2000); and DSM 5 (APA, 2013) with additional cultural context in glossaries of culture-bound syndromes and culture-specific disorders. In the early half of the last century, mental exhaustion among non-western students in West Africa with anxiety, affective and somatic symptoms have been syndromized as a unique cultural phenomenon referred to as the ‘Brain Fag Syndrome’ (Prince, 1960; APA, 2000; APA, 2013). More recently, some writers have generalized the presence of symptoms beyond Nigeria and West Africa to include African students in the diaspora. Numerous descriptions of this syndrome, replicated in scientific publications, books and other reference materials, claim the etymology of the term ‘Brain Fag’ (mental fatigue) is rooted in West African English both as an idiom of distress and explanatory model. This has also been widely replicated over the internet and in international educational curricula referencing the Diagnostic and Statistical Manual of the American Psychiatric Association (APA, 2000; APA, 2013). However, historical observations suggest precolonial use of the term within and across the Victorian British empire (Ayonrinde, 2008; Ayonrinde & Bhugra, 2014). In 19th century English, to be ‘fagged’ meant to be tired, whereas ‘fag’ in this context referred to fatigue, prostration, exhaustion or tiredness.
Suicidal ideation refers to suicidal thoughts. Suicidal ideation is described by ICD 11 as "thoughts, ideas, or ruminations about the possibility of ending one's life, ranging from thinking that one would be better off dead to formulation of elaborate plans (World Health Organization, 2020). The DSM-5 defines it as "thoughts about self-harm, with deliberate consideration or planning of possible techniques of causing one's own death (APA, 2013). Suicidal ideation is when one thinks about killing oneself. The thoughts might or might not include a plan to die by suicide. It is a risk factor to suicide in relation to active type suicidal thoughts. In literature, there is paucity of empirical studies associating Brain Fag Syndrome with suicidality. This suggests that BFS has not been considered a factor in suicide. This work contributes toward narrowing the gap. Assertiveness is a social skill that plays a pivotal role in ameliorating psychopathology. Assertiveness is the ability to speak up confidently and effectively for one's good in a socially responsible manner (Immanuel et al., 2023). Other scholars see assertiveness as self-confidence (Alberti & Emmons, 2008; Wolpe, 1958), ability to protect one's personal rights (Alberti & Emmons, 2008; Stein & Book, 2011), absence of anxious thoughts (Alberti & Emmons, 2017; Immanuel, 2019; Wolpe, 1958), respect for the rights of others and respect for one's own rights (Linehan, 1993). A lack of assertiveness is associated with several psychopathologies, including stress (Speed et al., 2017), anxiety (Immanuel. 2019; Janjani et al., 2020), depressive disorders as well as emotional instability, strained relationships, and low self-esteem (2017). The relationship between assertiveness and BFS has not been considered. Even though some empirical works have shown an association between assertiveness some mental disorders, none is reported for BFS. For instance, a lack of assertiveness is associated with several psychological problems, including stress, generalized anxiety, social anxiety, depression, and panic disorder, as well as emotional instability, strained relationships, and low self-esteem (Speed et al., 2017), but no such studies are reported for assertiveness and BFS either correlational, moderation or any other. It is the aim of the authors to make contribution in this area, seeing that brain fag is a contemporary prevalent mental health challenge. Assertiveness defined as the ability to express one's feelings, thoughts, and needs directly and appropriately, may serve as a moderating factor in the relationship between BFS and suicidal ideation. Individuals with higher levels of assertiveness are generally better furnished to manage stressors and seek support, potentially mitigating the psychological distress associated with BFS. By effectively communicating their challenges and setting boundaries, assertive individuals may reduce the likelihood of experiencing severe depressive symptoms and, consequently, suicidal ideation. It is expected that BFS positively predicts suicidal ideation. This is because mental strain when unabated could distort perception and precipitate suicidal thinking. It is also expected that assertiveness negatively predicts suicidal ideation since effective self-expression has a way of diffusing tension, and assertiveness could moderate the association of BFS and suicidal ideation, enabling individuals experiencing BFS to manage pressure more effectively, thus, abating suicidal cognition.
Participants
Participants in this study were two thousand seven hundred and forty-five (2, 745) persons from across the West African country of Nigeria. The authors sampled persons who volunteered and willingly responded to the online questionnaire. They included Men = 1,432 (52.2%) and Women = 1313 (47.8%); Age range 15-71, Mean Age was 28 years. Single participants were 1893 (69%), married = 666 (24%), cohabiting = 101 (3.7%), divorced = 58 (2.1%), and widowed = 27 (1%). Educational qualifications were as follows: Primary = 24 (.9%), high school = 284 (10.5%), undergraduates = 1, 248 (45.5%), graduates = 881 (32.1%), advanced degree = 241(8.8%) and others = 67 (2.4%). They were drawn from the major ethnic groups of the country, namely: Igbo = 2059 (75.0%), Hausa = 139 (5.1%), Yoruba = 189 (6.9%), others = 358 (13.8%).
Instruments
Brain Fag Syndrome Scale (BFSS): BFSS is a screening scale developed by Prince (1962) and refined by Morakinyo (1990). It has seven items. It assesses brain-fag syndrome. It has 3 response options of Never (0), Sometimes (1), and Often (2). Lowest score is 0, and highest score is 14, the higher the score, the higher the BFS. Examples of items in the scale are: “I find it difficult to concentrate when studying”, “These unpleasant sensations (burning, crawling, heat, cold) make it difficult for me to study or assimilate what I read”. In this study, Factor Analysis (Principal Component Analysis) was done, the eigenvalues was greater than 1.0 (3.33), and the Kaiser-Meyer Olkin measure of sampling adequacy was .84, the Bartlett’s test of Sphericity was 5740.41 (p<.000). One factor was extracted, and it explains 47.61% of the total variance. The BFSS is a unidimensional scale. Cronbach’s alpha is .70.
Positive and Negative Suicide Ideation-Negative Ideation (PANSI-NI): The Positive and Negative Suicide Ideation-Negative Ideation (PANSI-NI) is 8-item negative ideation sub-scale of the self-report measure of positive and negative thoughts related to suicidal attempts (Osman et al., 1998). Each item is rated using a 5-point scale ranging from 1 (none of the time) to 5 (most of the time). It measures risk of suicide. Cronbach’s alpha for the scale was α = .91 (Osman et al., 1998). In this study, the Cronbach’s alpha is .95.
Assertive Behavior Inventory: Assertiveness was measured with the 15-item Assertive Behaviour Inventory (ABI: Immanuel, 2019). It measures a person's ability to express one's needs, desires, and feelings honestly. Each item is scored on a five-point scale, with responses ranging from "Never (1) to "Always (5). Sample items include: "I compliment a person close to me for her/his beautiful appearance" and "I easily tell someone I love that I don't want sex". The author reported Cronbach's alpha coefficient of .84. In this study, Cronbach’s alpha = .80.
Procedure
The scales were distributed online and administered to two thousand, seven hundred and forty-five (2,745) participants in different regions in of the West African country. They filled the online form after they have given their consent to participate in the study.
Design/Statistics
The study adopted a cross-sectional design. This is a type of design in which data is collected from many people simultaneously. PROCESS Macro was used for data analysis. This is a test that analyzes the amount of variance explained in a dependent variable by predictor, as well as moderator variables.
Brain Fag Syndrome positively correlates with suicidal ideation (B=1.06, SE = .03; t=32.09, p < .000), indicating that as symptoms of Brain Fag Syndrome increase, suicidal ideation also increases. Assertiveness negatively correlates with suicidal ideation (B=-.31, SE = .01; t=-24.34, p < .000), suggesting that higher levels of assertiveness are associated with reduced suicidal ideation. Assertiveness moderates the association between Brain Fag Syndrome and suicidal ideation ((B=-.07, SE = .00; t=-20.55, p < .000), thus, weakening the positive association between BFS and suicidal Ideation. This indicates that assertiveness significantly moderates the relationship between Brain Fag Syndrome and suicidal ideation, suggesting that assertiveness acts as a buffer against suicidality. The model is significant, and explained 51% of the variance in suicidal behavior, F(3, 2741) = 960.45, p < .001.
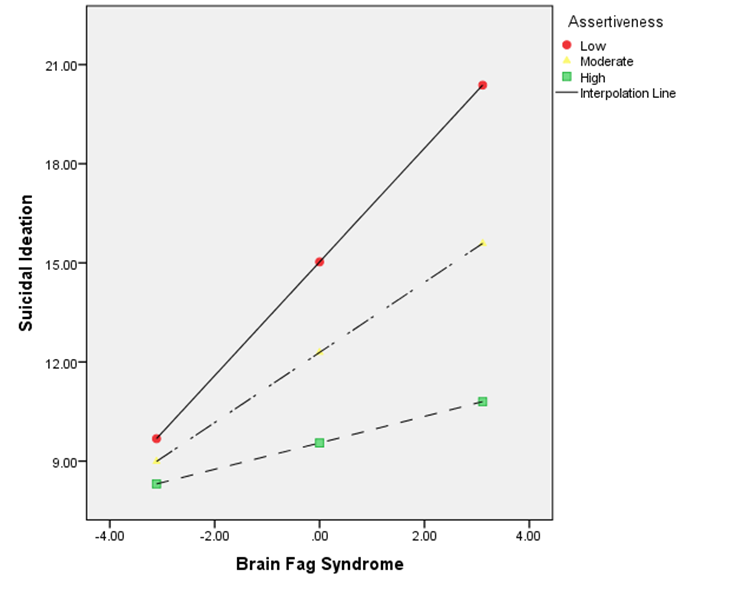
Figure 1: Graph depicting the interaction effect between Brain Fag Syndrome and Suicidal Ideation at various levels assertiveness. The interaction slope (Figure 1) revealed that the association between Brain Fag Syndrome and suicidal ideation varied depending on levels of assertiveness. At low assertiveness (red line: 8.88): The slope is steepest, indicating that individuals with low assertiveness show the strongest positive relationship between Brain Fag Syndrome and suicidal ideation, and the impact was significant (B = .40, SE = .05, t = 8.06, p < .001), confidence interval (95% CI=[.30, .50]).At moderate assertiveness (yellow line: .00): The slope is less steep than the red line, showing a reduced relationship between Brain Fag Syndrome and suicidal ideation compared to low assertiveness, and the impact was significant (B = 1.06, SE = .03, t = 32.09, p < .001), confidence interval (95% CI=[1.00, 1.13]). This indicates that people with moderate assertiveness who experience BFS were less likely to engage in suicidal cognition compared to those with low assertiveness.
Graph depicting the interaction effect between Brain Fag Syndrome and Suicidal Ideation at various levels assertiveness. The interaction slope (Figure 1) revealed that the association between Brain Fag Syndrome and suicidal ideation varied depending on levels of assertiveness. At low assertiveness (red line: 8.88): The slope is steepest, indicating that individuals with low assertiveness show the strongest positive relationship between Brain Fag Syndrome and suicidal ideation, and the impact was significant (B = .40, SE = .05, t = 8.06, p < .001), confidence interval (95% CI=[.30, .50]).At moderate assertiveness (yellow line: .00): The slope is less steep than the red line, showing a reduced relationship between Brain Fag Syndrome and suicidal ideation compared to low assertiveness, and the impact was significant (B = 1.06, SE = .03, t = 32.09, p < .001), confidence interval (95% CI=[1.00, 1.13]). This indicates that people with moderate assertiveness who experience BFS were less likely to engage in suicidal cognition compared to those with low assertiveness.
The findings of this study show that there is a positive association between BFS and suicidal ideation, indicating that as symptoms of Brain Fag Syndrome increase, suicidal ideation also increases. This is expected since high level of mental distress precipitate suicide. BFS is characterized by high level of mental confusion, pain and distress, and if unchecked, may likely orchestrate suicidal thinking. Further, there is a negative association between assertiveness and suicidal ideation, suggesting that higher levels of assertiveness are associated with reduced suicidal ideation. This is likely because assertiveness entails communication. As one communicates freely one’s needs in a socially responsible manner, it helps to ease up stress, thereby lowering the propensity for suicidal thinking. Furthermore, assertiveness moderates the relationship between BFS and suicidal ideation, weakening the positive association. Assertiveness in this sense acts as a buffer against suicidal thoughts. Prior to this study, there was no literature which had linked BFS and assertiveness. Assertiveness acts as a buffer. As assertiveness increases, the impact of Brain Fag Syndrome on suicidal ideation decreases. High assertiveness may provide individuals with better coping strategies, thereby reducing the effect of Brain Fag Syndrome on suicidal thoughts.
Psychopathology's influence on suicidality cannot be overlooked. Brain Fag Syndrome is a psychopathology. However, many individuals expressing suicidal thoughts are often diagnosed with mental health issues like Generalized Anxiety Disorder (Moffitt et al., 2007), post-traumatic stress disorder (APA, 2013), schizophrenia (Kasckow et al., 2011), depression (APA, 2013), substance abuse (Lemon, 2013), personality disorders (Hemelrijk et al., 2012), but rarely BFS. BFS is classified as a mental disorder according to DSM IV TR (APA, 2000) and DSM V (APA, 2013). A mental disorder is characterized by a clinically significant disturbance in an individual’s cognition, emotional regulation, or behaviour. Mental exhaustion associated with somatic sensations is common symptom of BFS. It is pertinent that health care professionals look out for the symptoms of BFS just like any other psychopathology in their clinical practice so that accurate diagnosis is made for better treatment outcome. Further, assertiveness is a beautiful communication skill, yet, it is deficient in many people. As the findings of this study reveal, assertiveness lowers the tendency for suicidal thinking, as well as mitigates the strength of BFS in degenerating to suicidality. This calls for integrating assertiveness training in healthcare services to people experiencing BFS so that they learn relevant communication skills that would enable them overcome their distress, and be integrated into society. This will benefit both the individual client and the community where they operate. The major limitation of this work is that it concentrated on a West African country. Future studies could collaborate with scholars from the Western countries such as North America and Europe as a step toward substantiating the idea of the global spread of the phenomenon of Brain Fag Syndrome.
Brain Fag Syndrome is a psychopathology. The BFS is positively associated with suicidal ideation. The moderation analysis demonstrates that assertiveness significantly moderates the relationship between Brain Fag Syndrome and suicidal ideation. As assertiveness increases, the effect of Brain Fag Syndrome on suicidal ideation weakens. This is a significant addition to literature that is almost silent on the phenomenon of BFS for decades. Factoring the BFS in healthcare screening and diagnoses, and finding treatment for the condition are tasks before mental health professionals.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
