AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2641-8975/015
1 Department of Pharmacology and Therapeutics, College of Health Sciences, University of Ilorin, Ilorin, Nigeria.
*Corresponding Author: Bodun Oye Olakanmi, Department of Pharmacology and Therapeutics, College of Health Sciences, University of Ilorin, Ilorin, Nigeria.
Citation: Olakanmi Bodun O, Olorundare Olufunke E, Afolabi Olanrewaju O, Njan Anoka, Akinola Olugbenga,Akanbi Olatunde A, Amase Nyanmgee, Adeneye Adejuwon A, Iwalewa Ezekiel O , Ntambi James M., Assessment of the Effects of Crude Methanolic Extracts (Leaf and Twig) of Loranthus micranthus on Streptozotocin Induced Diabetic Rats,J Diabetes and Islet Biology 2(1) Doi:10.31579/2641-8975/015
Copyright: © 2020 Bodun Oye Olakanmi This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 November 2019 | Accepted: 30 December 2019 | Published: 05 January 2020
Keywords: Loranthus micranthus, GC-MS, hyperglycemia, atherogenic index, pancreas, glycated-hemoglobin.
The antidiabetic effects of crude methanolic extracts of the leaf and twig of Loranthus micranthus was evaluated in Wister rats. To assess this, data were obtained for the determinant parameters of diabetic complications.
Streptozotocin was administered for induction of diabetes; diabetic state was confirmed by persistent hyperglycemia (FBG ≥ 300mg/dl) at 72 hours post induction. Invitro inhibitory activity on α- amylase and α-glucosidase was assayed. Serum insulin, TNF-α, Total cholesterol, HDL, LDL, TG, atherogenic index, liver glycogen and glycated haemoglobin were evaluated. Histology of the pancreas was assessed.
Phytochemical analysis revealed the presence of unique compounds in both extracts. In-vitro assay showed inhibitory effects of both extracts on α-amylase and α-glucosidase activity. Hyperglycemia was controlled in both extract-treated groups comparable to glibenclamide. Weight loss after diabetic induction was ameliorated in extracts treated groups; serum insulin level of the extracts-treated and glibenclamide treated-group were higher than the diabetic control group. Serum TNF-α level of extracts-treated and glibenclamide-treated groups were significantly lower than the diabetic control group. Glycated haemoglobin levels of diabetic control group were higher than the extracts treated and glibenclamide group. Dyslipidemia observed in the diabetic control group were ameliorated in all extract-treated groups; atherogenic index of diabetic control group was higher than extracts-and-glibenclamide treated groups. Histopathological assessment showed that the leaf and twig extracts of Loranthus micranthus may possess β cell regenerating activity.
Findings from this study suggest that the leaf and twig extracts of Loranthus micranthus ameliorate symptoms and complications of streptozotocin-induced diabetes in rats.

Graphical Abstract
Diabetes mellitus (DM) is a group of metabolic diseases characterized byhigh blood sugarlevels over a prolonged period (persistent hyperglycemia), due to defects in secretion of insulin or biologic action of insulin [1,2]. Prolonged diabetes causes many complications, which can be acute or chronic complications. Thesehas been linked to severe dysfunction and damage of various body organs: the eyes, kidneys, nerves, heart, blood vessels; and results annually in more than 5% deaths worldwide [3,1]. Persistent hyperglycemia has been reported to lead to the generation of free radicals through the formation of Schiff base and amadori products, which are implicated in the end organ damage caused by diabetes mellitus [4].
In 2017, it was estimated that 451 million (age 18-99 years) are living with diabetes worldwide [5]. These figures were expected to increase to 693 million by 2045 [5]. Approximately 5 million deaths worldwide were attributable to diabetes in 2017 within 20-99 years age range [6, 7]. The global healthcare expenditure on people with diabetes was estimated to be USD 850 billion in 2017 [8]. These new estimates of diabetes prevalence, deaths and healthcare expenditure present a large social, financial and health system burden across the world [5].
Diabetic patients with raised plasma glucose levels have proportionally more glycation occurring both intracellularly and extracellularly thereby necessitating the need to treat these complications as an integral part of the clinical stratification of diabetic patients [9,10]. Previous studies suggested that inhibition of the production of advanced glycated end products (AGEs) or blockade of their downstream signaling pathway to be promising targets for treatment of patients with diabetic complications [10,11,12,13].
One important complication of diabetes is the elevation of atherogenic risk, as diabetic dyslipidemia is a prominent contributor for the development of cardiovascular diseases [14]. Components of the immune system are altered in obesity and accompanying T2D, with striking changes occurring in the adipose tissue, liver, pancreatic islets, the vasculature and circulating leukocytes. These immunological changes include altered levels of specific cytokines and chemokines, changes in the number and activation state of various leukocyte populations, increased apoptosis and tissue fibrosis. Together, these changes suggest that inflammation participates in the pathogenesis of T2D [15, 16].
Conventional antidiabetic drugs are both costly and associated with many adverse effects [17]. Thus, the search for safer and affordable antidiabetic drugs has led to studies investigating several plants for such activity. Among plants with potent antidiabetic principles is the hemi parasite, Loranthus micranthus (L. micranthus) which is one of the species of African mistletoe found in Nigeria [18]. Mistletoe species show varying phytochemical components and bioactivity which is dependent on the host plant. The influence of the host tree on the antidiabetic activity has been reported by a group of researchers [18,19]. Studies have also shown seasonal variations in the antidiabetic activity of this semi parasite [20,21].African mistletoe parasitic on different host trees has been used for various medicinal purposes and ethnomedically as antidiabetic, antihypertensive and antimicrobial agent [22].
The aim of the present study is to evaluate the effect of crude methanolic extracts of leaf and twig of Loranthus micranthus separately, for their antidiabetic activities and their potentials in ameliorating some parameters of diabetic complications.
Fresh leaves and twigs of African mistletoe, Loranthus micranthus, were harvested during the dry season at Egbo Area in Ilaro, Ogun State, Nigeria. Plant identification was done at the Department of Plant Biology, University of Ilorin, Ilorin, Nigeria. A specimen was deposited at the herbarium and voucher number UILH/001/1260 was allocated to the sample. Plants materials were dried under the shade, at room temperature for 10days. The dried plants were separated into leaves and twigs and separately pulverized using mortar and pestle and weighed. The resulting powder was macerated in 95% methanol for 72hours.
2.2.Chemicals
Streptozotocin (STZ) (Sigma Aldrich, USA), p-nitrophenyl – α – d- gluco-pyranoside, p-nitrophenyl – β-d – glucopyranoside, α- glucosidase, α- amylase, carboxy methyl cellulose (Elabscience, UK), Elisa Rat insulin kit Elabscience, UK, Elisa Rat glycated hemoglobin kit, Elabscience, UK, Elisa Rat TNF-α kit, Elabscience, UK, HDL-Cholesterol Assay kit, Elabscience, UK, Cholesterol CHOD-PAP Assay kit, Elabscience, UK, Triglyceride GPO-PAP Assay kit, Elabscience, UK, Glycogen Assay kit (Sigma-
Aldrich), USA, Glibenclamide 5mg (Daonil), Aventis Pharma Ltd, Glucose, PBS, citrate buffer.
Cold maceration was used for the extraction, in which 1kg each of ground dried leaves and twigs were soaked in 3.5liters of 95% aqueous methanol. The set up was intermittently shaken vigorously for 72hours. The (residue) was removed by clarification using muslin which was discarded, and later filtered through Whatman No1 filter paper. The filtrates were then dried in-vacuo using a rotary evaporator at 400C. The resultant semi-solid was then concentrated on a water bath shaker at 400C for 60hrs.
3.Gas Chromatography Mass Spectrometer (GC-MS)
1.Gas Chromatography (GC) Analysis
Gas Chromatography (GC) analyses were performed on an Orion micromat 412 double focusing gas chromatography system fitted with two capillary columns coated with Cp-Sil 5 and Cp-Sil 9 (fused silica, 25µm × 0.25mm, 0.15µm film thickness) and flame ionization detector (FID). The volume of material injected was 0.2mL, and the split ratio was 1:30. Oven temperature was programmed from 50- 230OC at 3OC/min using helium as a carrier gas. Injection and detector temperature were maintained at 200 OC and 250 OC, respectively. Qualitative data were obtained by electronic integration of FID area percent without the use of correction factors.
2.4.2 Mass Spectrometry (MS) Analysis
In MS analysis, a Hewlett – Packed HP 5890A GC, interfaced with a VG analytical 70-250s double focusing mass spectrometer were used. Helium was used as the carrier gas at 1.2ml/min. The MS operating conditions were: ionization voltage 70ev, ion source 230OC. The GC was fitted with a 25m × 0.25mm, fused silica capillary column coated with Cp – Sil 5. The film thickness was 0.15µm; the GC operating conditions were identical with those of GC analyses. The MS data were acquired and processed by on-line desktop with a computer equipped with disk memory. The percentage compositions of the compounds were computed in each case of retention indices (determined relative to the retention times of series of n-alkanes) and mass Spectra with those of authentic samples and with data from literature [23,24].
2.5 Acute toxicity study
Twenty-four female Wistar rats divided into four groups receiving L. micranthus twig and leaf extracts at doses of 100, 250, 500 and 1000mg/kg daily for a period of 2 weeks. Each group consisted of three rats for each dose employed. The animals were observed during the first hour continuously and then every hour for six hours, thereafter at 12 hours and 24 hours. Animals were then observed every 24 hours for 2 weeks for any physical signs of toxicity such as writhing, gasping, palpitation and decreased respiratory rate or mortality.
6.Experimental Animals
Fifty-five (55) female rats, about 8 weeks old, weighing between 100-120g were used for the study. Animals were housed in Animal House Facility in the Central Research Laboratory, University of Ilorin, Ilorin, Nigeria, for 7 days under standard conditions of appropriate ventilation, temperature of 22-250C, relative humidity of 50% and 12hours day and night cycle. Animals were fed with standard rat chow and water was supplied ad libitum throughout the acclimatization period. Stressful conditions were avoided all through the experimental period.
7.Induction of Diabetes
Diabetes was induced in 40 rats by an intraperitoneal injection of a fresh solution of a single dose of streptozocin (STZ) Sigma Aldrich Chemicals, USA. The solution was prepared by dissolving STZ in 0.1M sodium citrate buffer, pH 4.5. Animals were administered with a dose of 65mg/kg body weight after been fasted overnight, according to the method described by Lenzen, 2008 [25]. Immediately after diabetic induction, animals were given 50% glucose solution in their drinking water ad libitum. Animals with fasting blood Glucose level (FBG) between 340 – 600mg/dl after 72hrs were considered diabetic and selected for the diabetic groups. For the purpose of treatment, the rats were randomly divided into the following experimental groups:
8.Experimental Groups
Group 1 = Normal control (n=5)
Group 2 = Normal rats + 500mg/kg leaf extract (n=5)
Group 3 = Normal rats + 500mg/kg twig extract (n=5)
Group 4 = Diabetic rats + 500mg/kg leaf extract (n=5)
Group 5 = Diabetic rats + 500mg/kg twig extract (n=5)
Group 6 = Diabetic rats + Distilled water (n=5)
Group 7 = Diabetic rats + 5mg/kg glibenclamide (n=5)
Group 8 = Diabetic rats + 250mg/kg leaf extract (n=5)
Group 9 = Diabetic rats + 250mg/kg twig extract (n=5)
Group 10 = Diabetic rats + 125mg/kg leaf extract (n=5)
Group 11 = Diabetic rats + 125mg/kg twig extract (n=5)
2.9 Body Weight Evaluation
Weights of the experimental animals were obtained at the beginning of the study- day 0, day 7, day 10 and day 14 of the experiment. Weights obtained were analyzed statistically.
2.10. Plasma Glucose Level
Plasma glucose level was determined by Accucheck plus GCT Glucometer (Roche, USA). The monitor of the glucometer device uses a reflectance photometer for measuring the intensity of the color formed at the end of the reaction. This measurement uses software which translated the intensity to the corresponding glucose values. The fasting blood glucose (FBG) of all animals was measured at day zero before diabetic induction to obtain baseline glucose level for all the rats; and thereafter, following the induction of diabetes and throughout the treatment period. Plasma glucose was determined 72hours after STZ injection for confirmation of diabetes. In addition, blood glucose was measured weekly for a period of 2 weeks using the glucometer method discussed earlier, following which the animals were sacrificed.
10.Oral Glucose Tolerance Test
Blood Glucose level of 16 hours fasted rats was determined, and the value used as zero time of the test. At the end of the experiment, i.e. after the last dose of the vehicle, or glibenclamide or extracts, glucose solution (50%) at a dose of 2g/kg was given by oral intubation, according to the methods described by Ayala et al., (2010) [26]. Blood samples were taken at 30, 60, 90 and 120 minutes after glucose loading and blood glucose level determined with one touch glucometer (Accucheck Plus GCT, Glucometer). Plots of the values of blood glucose level (mg/dL) versus the time intervals (min) were constructed and the area under the curve (AUC) calculated using the Trapezoidal method. The AUCs foreach group was compared and tested for significance against the diabetic-untreated group and this represented the tissue glucose utilization.
11.In-Vitro Antidiabetic Assays
2.11.1.α - Amylase Inhibitory Activity Assay
The effect of crude methanolic extracts of L. micranthus (leaf and twig) on α - amylase activity was determined by the method described by Ali et al., 2006 [27]. Briefly, 50µl of α- amylase (5U/ml) was pre-incubated for 20 min with 50µl aliquots of extracts. The reaction was started by the addition of 50µl starch (0.5%) dissolved in 20mM phosphate buffer at pH 6.9. The reaction mixture was incubated for a further 20 min at 370C and the catalytic reaction terminated by addition of 2.0 ml of DNS reagent (1% 3, 5-dinitrosalicicyclic acid (DNS) and 12% sodium potassium tartrate in 0.4 M NaOH). The reaction mixture was heated for 15 min at 100oC. α-amylase activity was determined by spectrophotometric measurement of the absorbance at 540 nm. Percentage α-amylase inhibition was calculated according to the following formula;
(A0 – A1) / A0 x 100 where, A0 was the absorbance of the control (blank, without extract) and A1 was the absorbance in the presence of the extract.
2.11.2. α - Glucosidase Inhibitory Activity
The inhibitory effect of L. micranthus extracts on α-glucosidase activity was determined according to the chromogenic method described by Kim et al. (2005) [28]. Briefly, α-glucosidase (5 units) was pre-incubated with 20 µg/ml of the different extracts for 15 min. Para-nitrophenylglucopyranoside (PNPG) (3mM) dissolved in 20 mM phosphate buffer, pH 6.9, was added to start the reaction. The reaction mixture was further incubated at 37oC for 20 min and stopped by addition of 2 ml of 0.1 M Na2CO3. Using a spectrophotometer, the α-glucosidase activity was determined by measuring the yellow colored p-nitrophenol released from PNPG at 400 nm. Percentage α-glucosidase inhibition was calculated according to the following;
(A0 – A1) / A0 x 100 where, A0 was the absorbance of the control (blank, without extract) and A1 was the absorbance in the present extract.
11.Sample Collection and Handling
At the end of the 14-day treatment blood samples were drawn 3 hours after the last dose from the orbital sinus of rats, under light ether anesthesia into two different tubes (heparin and plain bottles) for each animal respectively. The samples were immediately centrifuged at 0oC/1000g for 15min for separation of serum. The resulting serum samples was separated and kept at -200C until used for required analysis.
2.13. Estimation of Plasma Insulin Level
Insulin concentration was determined by radioimmunoassay procedure using a Rat INS (Insulin) ELISA Kit (Elabscience, E-EL-R2466, 96T). This assay has a high specificity as it recognizes natural and recombinant Rat INS without significant cross-reactivity or interference between Rat INS and analogues. The ELISA kit uses Sandwich-ELISA as the method. Sample and reagent preparation was done according to the manufacturer’s manual using serum samples. Spectrophotometric measurements were done at a wavelength of 450 nm ± 2 nm. Concentration of insulin in the samples was calculated by comparing the OD of the samples to the standard the curve.
14.Estimation of Tissue Glycogen
At the end of the experiments, livers collected were weighed and divided into 2 sample tubes, for liver glycogen assay and histopathological evaluation. Liver samples for glycogen assay were immediately frozen in phosphate buffered saline prior to the assay. Glycogen content of liver was assayed using glycogen assay kit (Sigma-Aldrich, 3050 Spruce Street, ST. Louis, MO 63103 USA). The coupled enzyme assay produces a colorimetric (570 nm) product, proportional to the glycogen concentration present in the samples.
2.15. Estimation of Plasma Lipid Profile
Blood lipid (TC, HDL and TG) levels were determined using spectrophotometric assay techniques. Assays were conducted according to the manufacturer’s manual. Serums of all the animals in different groups were analyzed.
2.15.1 Total Cholesterol
Total cholesterol in serum was assayed using Elabscience Total Cholesterol Assay Kit. The assay is based on the enzyme driven reaction that quantifies both cholesterol esters and free cholesterol. Cholesterol esters were hydrolyzed via cholesterol esterase to cholesterol, which was subsequently oxidized by cholesterol oxidase to the ketone cholest-4-en-3-one and hydrogen peroxide. Hydrogen peroxide was detected with a high specificity colorimetric probe. Horseradish peroxidase (HRP) catalyzes the reaction between the probe and hydrogen peroxide, which was bound in a 1:1 ratio. Samples were compared to a known concentration of cholesterol standard in a 96-well microtiter plate. Samples and standards were incubated for 45 mins and then read on a standard 96-well colorimetric plate reader, at absorbance of 540 nm. The concentration of cholesterol in each sample was calculated by comparing the sample absorbance values to the cholesterol standard curve.
Sample corrected absorbance
________________________________
Total Cholesterol (μM) = Slope x Sample dilution
2.15.2. Serum Triglycerides Concentration
Triglycerides level in serum was assayed using GPO-PAP method (Elabscience TG Assay Kit).All reagents were ready to use and were mixed according to the manufacturer’s manual. The mixture was measured after incubating at 370C for 5 min. Absorbance of sample against reagent blank was read at 550nm within 60 min. Triglycerides concentration in the sample was calculated as follows:
A samplex concentration of Standard = Triglycerides concentration
A Stand
(where Asample and Astandard: absorbance of sample and standard respectively)
2.15.3. High Density Lipoprotein Cholesterol (HDL-C) Assay
High Density Lipoprotein Cholesterol (HDL-C) in the serum of each sample was assayed according to the manufacturer’s manual using direct method, with Elabscience High Density Lipoprotein Cholesterol (HDL-C) assay kit. 10µl of serum was mixed with reagents R1 and R2. The solutions were mixed thoroughly and incubated at 370C for 5 minutes. The absorbance was read at 546nm wavelength. HDL Cholesterol concentration in the samples was calculated according to the calculation formula in the manual.
(Absorbance of sample– Blank) X concentration of standard = HDL-C concentration
____________________
(Absorbance of standard – Blank).
2.15.4. LDL Cholesterol
LDL-Cholesterol was estimated by using the formula of Friedewald et al., 1972 [29]:
LDL – Cholesterol = Total cholesterol –HDL-Cholesterol – TG/5.
2.15.5. Atherogenic Index
The Atherogenic index (AI) was calculated according to the formula of Harnafiet al., 2014 [30].
AI = Total Cholesterol – HDL-Cholesterol
____________________________
HDL – Cholesterol
2.16.Glycated Hemoglobin (HbA1c)
Glycated hemoglobin was assayed from the whole blood usingHbA1c ELISA kit (Elabscience) which employed the competitive enzyme immunoassay technique, utilizing a monoclonal anti-HbA1c antibody and an HbA1c-HRP conjugate. The intensity of color formed was measured spectrophotometrically at 450nm on a microplate reader. The intensity of the color was inversely proportional to the HbA1c concentration. A standard curve was plotted relating the intensity of the color (O.D.) to the concentration of standards. The HbA1c concentration in each sample was determined from this standard curve.
2.17. Tumor Necrotic Factor-Α (TNF-α)
TNF-α was assayed using rat TNF-α ELISA Kit (Elabscience, E-EL-R0019).Standards and samples were prepared according to the manufacturer’s specification. The prepared solutions were added to the appropriate micro ELISA plate wells and combined with specific antibody for TNF-α and Avidin-Horseradish Peroxidase (HRP) conjugate and were incubated. The free unbound components were washed away. Only the wells that contained TNF-α, biotinylated detection antibody and Avidin-HRP conjugate appeared blue. The enzyme-substrate reaction was terminated by addition of H2S04 which turned the blue colour yellow. The optical density (OD) was measured spectrophotometrically at a wavelength of 450nm. The OD values obtained were proportional to the concentration of TNF-α in each microplate well. The concentration of TNF-α in the samples was calculated by comparing the OD of samples was determined from the standard curve.
18.Histopathology
Pancreas and pancreatic tissues within the duodenal loop of each rat in all groups were taken out immediately after animalswere sacrificed, at the termination of the experiments. These were fixed in 10% phosphate buffered formaldehyde solution for at least 48 hours. The tissues were later cut into 0.5x1cm in diameter each using scalpel blade and processed using an automatic tissue processor. Processed tissues were embedded using MP3 tissue embedding center. A rotary microtome machine was used to section at 5 μm. Hematoxylin and eosin (H&E) stain was used for staining sections which were mounted using dextrin plasticizer xylene (DPX). For histopathological examination, low and high powered field of Carl Zeiss® binocular microscope was used.
2.19.Statistical Analysis
Data obtained in the present study were subjected to statistical analysis using GraphPad Prism application version 6. The means, standard errors of means and standard deviations were obtained as summary statistics. The obtained summary statistics were subjected to one-way analysis of variance (ANOVA) using the Tukey’s post-hoc test to check for significant relationship between experimental groups. The data were pictorially presented as line graphs and bar charts with bars and error bars representing the means and standard errors of means respectively. Statistical significance was set at p value less than 0.05.
Qualitatively, 48 and 40 compounds were found to be prominent in leaf and twig extract of L. micranthus respectively. Thirteen of the compounds were commonly found in both leaf and twig of L. micranthus. The similar compounds are Cyclobutanol, 1,4- Dimethyl hexyl alanine, Piperazine, 4-Butyl phenol, N-(2-Hydroxy benzyl) alanine, Palmitic acid methyl ester, Ethyl hexadecanoate, 2- Undecyl phenol, Phytol, Methyl stearate, Methyl linoleate, Ethyl oleate and Squalene.
Quantitatively, Palmitic acid methyl ester, Phytol, Methyl stearate and Methyl linoleate were found in higher quantity in the leaf than the twig extracts of L. micranthus. However, Cyclobutanol, 1,4- Dimethyl hexyl alanine, Piperazine, 4-Butyl phenol, N-(2-Hydroxy benzyl) alanine, Ethyl hexadecanoate, 2- Undecyl phenol, Ethyl oleate and Squalene were found in significant amounts in the twig compared to the leaf extract of African Mistletoe.
3.2 Mean Body Weight
| (%)Mass Spectra Functional Compounds S/N | R.I | Composition Data | Group |
| Cyclobutanol | 668 | 27 39 44 57 70 | -OH |
| Methoxyoxirane-2- | 827 | 0.3 29 45 58 73 87 -COOH - | -C-O-C Carboxylic acid |
| Ethyl trans-3-methyl-2- carboxylate | 837 | 0.3 27 29 4557 74 -C-O-C | Oxirane |
| l-Alanine, trimethylsilyl ester | 874 | 44 59 75 86 103 | NH2, -COO, |
| Neoheptanol | 875 | 57 73 85 101 115 | -OH |
| Vinyl2,2-dimethyl Butanoate | 889 | 41 4357 71 85 | |
| 1,4-Dimethyl hexylamine | 931 | 0.1 445670 97 114 | -NH2 |
| Piperazine | 1011 | 28 4456 83 85 | -NH |
| Coumaran | 1036 | 63 77 91 105120 | -C=O,-C=C |
-limonene diepoxide | 1128 | 41 43 6783 95 | -C-O-C |
| -Campholenal | 1153 | 81 93 108 119 137 | -CHO, -C=C |
| 2-Propyl malonicacid | 1266 | 41 44 6073 87 | -COOH |
| D-2-Deoxyribose | 1274 | 27 31 4457 73 | -OH,-C=O |
| P-butyl phenol | 1312 | 77 91 107121 123 | OH,-C=C |
| 2,3-Bis(1,methylallyl) | 1328 | 82 97 124 126 150 pyrollidine | -NH |
| 3-Butyl indolizidine | 1393 | 96 110 124138 152 | -NH |
| P-Coumaric alcohol | 1464 | 94 107121 131 150 | -OH, -C=C |
| Methyl alpha-L-fuco | 1471 | 43 60 74 87 100 | -OH pyranoside |
| 2,3-Dimethyl- 2(3- oxobutyl) | 1521 | 41 4369 82 97 | -C=O |
| Trimethyl[1-methyl | 1533 | 73 87 101 117 129 | dodecyl)oxy] Silane |
| Methyl isomyristate | 1615 | 57 74 87101 115 | -COO Cyclohexanone |
| 3-Oxo-alpha-ionol Methyl 3,4, trimethoxy Benzoate | 1627 1628 | 79 95 108123 137 155 168195 196 226 | -OH, -C=O -C=C C=C |
| Methyl tetradecanoate | 1715 | 41 55 57 7487 | -COO |
| Hexahydrofarnesyl acetone | 1754 | 41 4358 71 85 | -C=O |
| Sulfurous acid,isohexyl | 1773 | 83 85 101 137 167 | Hexyl ester |
| Methyl pentadecanoat | 1779 | 57 7487 101 115 | -COO |
| N-(2-Hydroxybenzyl) | 1803 | 4456 77 95 107 | alanine |
| Palmiticacid, methylester | 1878 | 57 7487 101 115 | -COO |
| 3,5,11,15-Tetramethyl-1- Hexadecen-3-ol | 1899 | 57 71 95109 123 | C=C, -OH |
| Farnesyl acetone | 1902 | 41 43 6981 95 | -C=O |
| Heptadecanoic acidmethyl | 1978 | 57 7487 101 115 | -COO ester |
| Ethyl hexadecanoate | 1978 | 57 73 88101 115 | -COO |
| 2-Undecyl phenol | 2008 | 77 91 107 121 131 | -OH,-C=C |
| Phytol | 2045 | 41 57 71 95 111 | -OH |
| Methyl stearate | 2077 | 41 43 74 87 101 | -COO |
| Methyl linoleate | 2093 | 41 55 67 81 95 | -COO |
| Ethyl oleate | 2185 | 4155 69 83 88 | -COO |
| Methyl-18-methyl nona | 2212 | 57 74 87101 115 | -COO decanoate |
Table 1 Shows the identities, retention indices, percentage composition and mass spectra data of the constituents of methanolic extract of L. micranthus. In the Table, 48 compounds were identified from their mass spectra, the number represented 94.9% of the leaf.

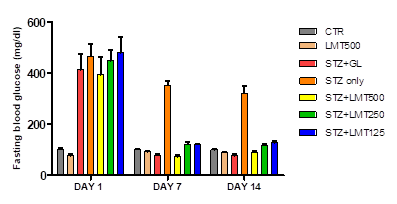
Treatment groups (Glibenclamide, LML and LMT extracts) showed adequate glycemic control at all concentrations used. CTR= control, LML= L. micranthus leaf extract, LMT= L. micranthus twig extract, STZ= streptozotocin, GL= glibenclamide.
* is p value < 0.05 relative to controlgroup. Data is presented as mean (bars) ± standard error of mean (error bars).
3.3.1. In Vitro Assay
The inhibitory activity of the leaf and twig extract of L. micranthus on α-amylase and α-glucosidase enzyme activity were evaluated in vitro at different extractconcentrations. The result obtained was analyzed and are presented in the line graphs below.
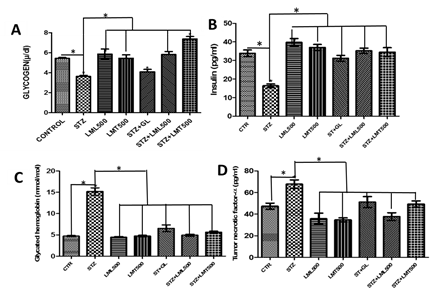
CTR= control, LML= L. micranthusleaf extract, LMT= L. micranthus twig extract, STZ= streptozotocin, GL= glibenclamide. Data is presented as mean (bars) ± standard error of mean (error bars). * is significant level of p< 0.05 relative to the STZ group.
LIPID PROFILE
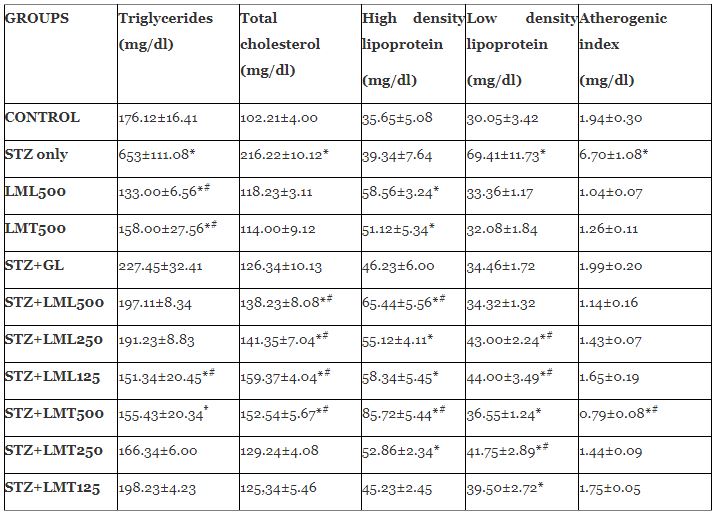
STZ-only group showed significantly higher (p<0.05) TC compared to other groups. TG level is significantly higher (p<0.05) in STZ-only group compared to GL, LML and LMT treated groups. LML treated groups showed significantly higher HDL compared to other groups other treatment groups. LDL is significantly higher (p< 0.05) in STZ only group compared to all treatment groups. STZ-only group showed significantly higher (P<0.05) AI compared to all treatment groups. STZ+LMT500 treated group showed significantly lower (p<0.05) AI than all other groups.
3.3 ORGAN WEIGHT
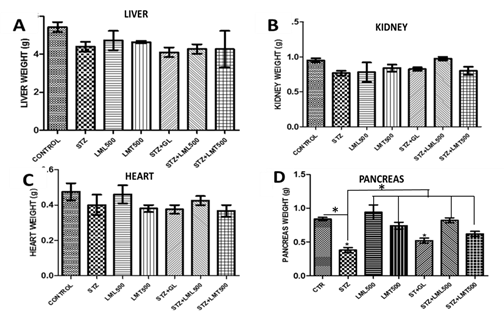
CTR= control, LML= L. micranthus leaf extract, LMT= L. micranthus twig extract, STZ= streptozotocin, GL= glibenclamide.
* and # are p value >0.05 relative to control. Data is presented as mean (bars) ± standard error of mean (error bars).
3.5 Histopathological Observations
Following tissue microscopic examination, pancreatic tissues from all animals were evaluated and it was observed that the control group pancreas showed normal architecture, with intact acinar cell cytoplasmic and nuclear structures. In rats administered 65mg/kg body weight STZ to induce a diabetic state, it was observed that there was severe diffuse necrosis of both exocrine and endocrine pancreatic tissues. Although, the diabetic group treated with glibenclamide in a bid to reverse the destructive effect of Streptozocin treatment showed some multifocal pancreatic necrosis, overall, the animals in this group showed severe acinar (exocrine) nuclei hyperchromasia, possibly an indication of increased acinar cells’ nuclei activity. The pancreas of STZ induced diabetic rats treated with L. micranthus leaf extract showed mostly normal acinar cells (figure 1D). The pancreas of STZ induced diabetic rats treated with L. micranthus twig extract showed bridging pancreatic necrosis admixed normal acinar regions (figure 1E), implying normal pancreatic tissue admixed necrotic tissue.

Diabetes mellitus (DM) is a serious chronic disease, with heavy cost implication on human population globally [8]. This has heightened the search for alternative therapies with potentially low toxicity, and hence better safety profile, for the treatment of the disease, to improve the quality of life of diabetic patients, and/ or reverse diabetic complications.
Gas chromatography – mass spectrophotometric (GC-MS) analysis showed the presence of different compounds in the twig and leaf extract at varying concentrations. This suggests that the presence of these compounds could be contributory to their unique antidiabetic activity. Leaf extract showed the presence of higher concentration of palmitic methyl ester which has been reported to possess several antidiabetic properties including activation of peroxisome proliferator-activated receptor (PPAR) family [31] and inhibition of α-amylase and α- glucosidase [32]. Other components such as Thymol, linmonene, camphor, and benzoic acid derivatives, have shown good antioxidant and antidiabetic potentials [33, 34, 35].Thirteen compounds were found to be common in both leaf and twig extract of L. micranthus.
Acute toxicity study of both the leaf and the twig extract showed that both were safe at the maximum concentration (2000mg/kg body weight) employed. This finding supports previous safety study on L. micranthus [36]. This showed that the methanolic extracts of the both leaf and twig of L. micranthus are safe at the doses administered to the animals.
One of the mechanisms of action of antidiabetic agents include: causing reduction in glucose absorption from the gastrointestinal tract (GIT) [37]. This was assessed by evaluating the in vitro inhibitory effect of LML and LMT on starch degrading enzymes (α-amylase and α- glucosidase). Clinically used antidiabetic drugs, such as Acarbose and miglitol inhibit both enzymes and reduce the rate of digestion of complex carbohydrates but this is accompanied by gastrointestinal discomforts [38]. Management of blood glucose level is a critical strategy in the control of diabetes and its complications, this makes leaf and twig extracts of L. micranthus potential candidates for controlling glucose release at GIT level. Both extracts could prevent postprandial spikes that have been implicated in cardiovascular and macro-vascular complications of diabetes[39].The twig extract showed better inhibitory effect on α-amylase and α-glucosidase compared to the leaf extract.
STZ-induced hyperglycemia was established in all diabetic groups in order to evaluate the effect of LMT and LML on treatment groups. The significant weight loss (p<0.05) in all STZ-induced diabetic groups could be strongly linked to STZ-induced destruction of beta cells of the islets of langerhans of the pancreas; the attending abolition of insulin production and secretion, and resultant decreased glucose uptake and storage [40,41]. The destruction of the pancreas resulted in utilization of non-carbohydrates nutrients such as proteins and fatty acid for the synthesis of glucose. The loss of structural proteins as a result of increased gluconeogenesis together with increased glycolysis and increased synthesis of ketone bodies results in severe weight loss in diabetic animals [40, 41]. L. micranthus extracts- and- glibenclamide treated groups showed similar weight gain pattern which is indicative of the ameliorating effect of the treatments on weight loss in STZ-induced diabetic rats. The effects of the extracts in ameliorating STZ-induced weight loss has been reported for borneol, cavarcol and Swertianmarine [42,43,44]. Twig and leaf extract of L. micranthus may contain principles useful in ameliorating weight loss seen in Type-1 DM.
Persistent hyperglycemia is a major factor in the pathophysiology of DM. Hypoglycemic agents should possess the ability to reduce the fasting blood glucose in diabetic patients. From the presents study, the fasting blood glucose of all animals in different groups at the start of the experiment were not significantly different (p>0.05). After induction of diabetes, the diabetic groups showed significant hyperglycemia which could be attributed to destruction of pancreatic beta cells, causing reduction in insulin production and hence, poor glucose utilization. The result showed adequate control of hyperglycemia in the glibenclamide-treated group and the L. micranthus leaf and twig-extract treated groups. The hypoglycemic effect of the extracts was observed at day 7 of treatment, and was consistent up to day 14 of treatment, suggesting that the extracts could be used for management of DM-induced hyperglycemia. This is consistent with the previous studies in alloxan-induced diabetes [45,46].
The effect of glibenclamide, LML and LMT on glucose utilization assessed by the oral glucose tolerance test (OGTT) exhibited comparable glucose utilization pattern to normoglycemic group. This showed that both leaf and twig extracts of L. micranthus had similar effect on glucose utilization comparable to glibenclamide (p<0.05).
DM impairs glycogen synthesis both in the rat’s liver and skeletal muscles [47]. The glycogen content of skeletal muscle and liver are markedly decreased in DM [48]. Result of the present study showed increase in the liver glycogen content of all extract-treated animals compared to the diabetic untreated group. LMT treated animal showed significantly (p<0.05) higher liver glycogen levels compared to other groups. Normal control group, LML500 and STZ-LML500 groups showed similar liver glycogen levels. This showed that the leaf and twig extracts of L. micranthus could improve glycogen storage possibly by inducing glycogenesis or reducing glycogenolysis in DM. This activity has been reported for borneol, citornellol and mytenal [42, 49, 50, 51] which were monoterpenes derived from different plants with antidiabetic activities.
The damaging effect of streptozotocin on pancreatic beta cells resulted in reduction in the level of serum insulin of the diabetic untreated rats compared to the control, glibenclamide-treated and L. micranthus extract-treated diabetic rats. LML500 treated diabetic rats showed higher serum insulin level than glibenclamide (an insulin secretagogue. [52] and LMT 500. Thus suggesting that leaf extract of L. micranthus has better insulin-secreting activity than the twig and glibenclamide-treated group. The result correlate with the findings of Gray and Flatt [53].
LML500 and LMT500 extracts had significantly higher (p<0.05) effect at reducing haemoglobin glycation comparable to glibenclamide. Clinical studies have shown that glycated hemoglobin is higher in diabetic patients than in non-diabetic individuals [54]. In the present study, reduction in haemoglobin glycation by the extracts could also be attributed to the activity in stimulating insulin secretion, or increasing glycogenesis and glucose utilization, leading to reduced blood glucose level and reduction in the rate of haemoglobin glycation. In addition, the antioxidant effect on phytochemicals in L. micranthus extracts similar to what was reported for D-limonene and thymol in previous studies [55,56] could play a role.
The role of tumor necrotic factor-α (TNF-α), an adipocytokine in systemic inflammation has been established in DM [57,58]. LML500 and LMT500-treated diabetic group showed a significantly lower (p< 0.05) TNF-α level compared to all other groups. Results from the present study also showed that L. micranthus leaf extract exhibited better serum TNF-α lowering effect than glibenclamide. The leaf and twig extracts of L. micranthus may reduce diabetic complications by exerting anti-inflammatory activity and lowering levels of TNF-α in inflammatory and metabolic diseases such as DM. Similar effect has been reported in adipocytes for geniposide [59].
Dyslipidemia is a critical feature of uncontrolled DM, characterized by high total cholesterol (TC), low density lipoprotein (LDL) cholesterol and triglycerides, and a reduction in the level of high density lipoprotein (HDL) cholesterol [14]. Acute insulin deficiency initially causes an increase in free fatty acid mobilization from adipose tissue resulting in an increased production of LDL cholesterol particles and resultant dyslipidemia [60, 61, 62]. LML500 and LMT500 showed similar control of the TC, LDL and serum triglyceride level at all doses used. Similarly, hypercholesterolemia observed in diabetic-untreated groupwere lowered in glibenclamide, LML and LMT treated groups. In addition, HDL cholesterol level was significantly increased (p<0.05) in extract-treated animals than glibenclamide-treated group. Thus, suggesting a role for the extracts in the management of diabetic-induced dyslipidemia. Similar effect has been reported for D-Limonene and thymol [44, 55]
Atherogenic index is a predictor of atherosclerosis, resulting from the imbalance between HDL and total cholesterol. Atherosclerosis is a major contributor to the global morbidity and mortality, both in hypertensive and diabetic individuals [63, 64]. LML-treated groups showed atherogenic index significantly lower (p<0.05) than the glibenclamide treated group. The extracts showed potent antidyslipidemic effect. The extracts may therefore be useful at reducing the risk of cardiovascular, and vascular events and death that are complications of chronic DM.
Analysis of weight of organs showed no significant difference (p>0.05) in the weight of the liver, heart and kidney of all experimental groups. Weight of pancreas for the STZ-diabetic untreated group was significantly lower (p<0.05) compared to weights of the pancreas in all other experimental groups. The increase in the weight of pancreas of LML500 treated group suggests that LML contain active phytochemicals that are capable of regenerating pancreatic beta cells. Further studies are required to confirm this finding.
The histopathological photomicrograph of the pancreas of experimental animals in this study re-enforces the destructive nature of STZ on both exocrine and endocrine pancreatic tissues, as it caused necrosis in these tissues. Also, the efficacy of glibenclamide in the treatment/management of diabetic state was shown to be partly due to increased activity of the islet and acinar cells which in the present study were observed to be hyperchromatic. This study demonstrates the ameliorating effect of L. micranthus leaf and twig extracts on the STZ- induced destruction of acinar and beta cells of the pancreas. Similar effects has been reported for menthol and palmitic acid ester [31, 51, 65].
In conclusion, this study showed the therapeutic benefits of L. micranthus in management of, and prevention of complications of DM via different mechanisms. Further studies are required to identify the phytochemical principles responsible for these antidiabetic actions and their possible mechanisms of action tested.
We acknowledge the staff of Central Research Laboratory, Animal House and Chemical Engineering Department, University of Ilorin, Ilorin for their contributions to this work. We also acknowledge Mr Femi Adesua of Department of Pharmacology and Therapeutics, University of Ilorin, Ilorin for his contributions in the extract preparation.
5.0 Conflict of Interest
The authors of this manuscript declare that there is no conflict of interest
6.0 Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or
Not-for-profit sectors.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.
Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti
