AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-4861/416
Tex St. Cyril and St. Methodius University of Veliko Tarnovo Veliko Tarnovo 5003, Teodosii Tarnovski St., 2, Bulgaria
*Corresponding Author: Antoaneta Vacheva, Tex St. Cyril and St. Methodius University of Veliko Tarnovo Veliko Tarnovo 5003, Teodosii Tarnovski St., 2, Bulgaria.
Citation: Antoaneta Vacheva, (2024), Influence of Personal Factors on Quality of Life in Patients with Chronic Obstructive Pulmonary Disease (COPD), International Journal of Clinical Case Reports and Reviews, 17(1); DOI:10.31579/2690-4861/416
Copyright: © 2024, Antoaneta Vacheva. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 March 2024 | Accepted: 21 March 2024 | Published: 04 April 2024
Keywords: chronic obstructive pulmonary disease; anxiety; negative affectivity; social inhibition
Chronic Obstructive Pulmonary Disease (COPD) is a disease characterized by restriction of airflow in airways. Smoking is a major risk factor for disease. Other factors are air pollution from fuels, industrial dust, chemical agents and genetic causes. Main symptoms are shortness of breath, chronic cough with or without sputum and rapid fatigue. Chronic obstructive pulmonary disease /COPD/ is a source of stress and anxiety, due to severity of disease, need for long-term treatment and detachment from social life. Study cohort consisted of 124 patients with a diagnosis of COPD and a control group of 162 without lung disease. Persons studied are over 18 years of age, of different sexes, of Bulgarian ethnic origin and different family and social status. Chronic obstructive pulmonary disease is a disease of increasing social importance and, according to forecast of WHO, by 2030 it is expected to become third leading cause of death in world. Aim of pilot study was to determine influence of some personal risk factors (anxiety and type D personality in dimensions: "negative affectivity" and "social inhibition") on quality of life and social adaptation of patients with COPD.
Chronic obstructive pulmonary disease (COPD) is a progressive disease characterized by long-lasting respiratory symptoms and airflow limitation.[3] Global Initiative on Chronic Obstructive Lung Disease (GOLD) 2024 defines COPD as a heterogeneous lung disease characterized by chronic respiratory symptoms (difficulty breathing, cough, sputum production, chest pain, wheezing) due to airway abnormalities (bronchitis, bronchiolitis). or alveoli (emphysema), which often cause progressive airflow obstruction.[4] Main reason for occurrence and development of chronic obstructive pulmonary disease is smoking /active and passive.[8] Other risk factors for developing COPD are air pollution from dust, fumes or chemicals, indoor air pollution from biomass fuel (wood, animal dung, crop residues), coal in home, poor growth in womb, prematurity, frequent or severe childhood respiratory infections, childhood asthma, genetic disease - alpha-1 antitrypsin deficiency.[2] Emphysema is a structural abnormality with enlargement of air spaces (alveoli) whose walls have collapsed, resulting in permanent damage to lung tissue with or without limitation of airflow. Chronic bronchitis is defined as a productive cough.[5][6] Chronic bronchitis does not always lead to airflow limitation, but adults with chronic bronchitis who smoke are at high risk of developing COPD.[7] Emphysema and chronic bronchitis remain predominant phenotypes of COPD. COPD usually occurs in men and women over age of 35-40.[1][3] Chronic Obstructive Pulmonary Disease (COPD). COPD is fourth leading cause of death worldwide. According to WHO data, COPD kills over 3 million people every year, with over 90% of registered cases with a fatal outcome concentrated in low- and middle-income countries.[9][10]. Chronic obstructive pulmonary disease is a disease of increasing social importance and, according to forecast of the WHO, by 2030 it is expected to become third leading cause of death in world. [11]. European Union presents data on COPD as a component of nosology "Diseases of the respiratory system". Eurostat indicates that in Community, deaths from respiratory diseases account for 7.5% of all deaths [12], making respiratory diseases third most common cause for death in EU after CVD and malignant neoplasms.[13] According to WHO data, 251 million people in world suffer from COPD, and forecasts show an increase in the prevalence of disease in coming years.[14] Official statistics of Ministry of Health indicate that in 2018, between 5 and 10% of Bulgarians are sick with COPD, only 75,000 of them are being treated. Specialists believe that frequency of COPD in our country is significantly above European average and covers more than 10% of the population over 40 years of age.[15] Dr. Samuel Kutash, an American clinical psychologist and professor of psychology, developed a theory of anxiety using research on anxiety and stress. According to Dr. Kutash, “Anxiety or a state of disequilibrium occurs when a person does not experience an optimal level of stress for their own constitution. Tranquility or a state of equilibrium or under-equilibrium occurs as a result of experiencing an optimal level of stress for one's own structure either in healthy balance (equilibrium) or in unhealthy balance (under-equilibrium).[16]
Aim of pilot study
Аim of pilot study was to determine the influence of some personal risk factors (anxiety and personality type D in dimensions: "negative affectivity" and "social inhibition") on the quality of life and social adaptation of patients with COPD.
Tasks
1. To investigate the elements of quality of life in patients with COPD related to self-rated health, exercise, self-care and activities of daily living.
2. To investigate some risk factors and personality characteristics for type D in patients with COPD.
3. To investigate the relationships and dependencies between quality of life, anxiety and type D personality in patients with COPD.
Hypothesis
It is allowed that patients with COPD, with a higher level of anxiety and higher D personality scores, will have a worse quality of life and social adjustment.
Logical units of observation
✓ Patients diagnosed with COPD: mild COPD; moderate COPD; severe COPD; very severe COPD.
✓ Control group of individuals without lung disease
Factorial signs of observation:
➢ Demographic: gender; age; education; marital status; labor activity.
➢ Health status: duration of illness; risk factors: smoking
➢ Spheres of health-related quality of life: mobility; self-service; usual activities; pain/discomfort; anxiety/depression; self-rated health;
➢ Personal anxiety;
➢ Type D personality:
• negative affectivity;
• social isolation.
➢ Social adaptability.
Sociological methods
Self-assessment questionnaires
➢ Standardized questionnaire for health-related quality of life research - EQ-5D-3L; adapted Bulgarian version.
➢ Questionnaire for determining belonging to personality type D - (D Scale -14); adapted Bulgarian version.
➢ Questionnaire for the study of personal anxiety - Trait Anxiety Inventory; adapted Bulgarian version.
Statistical methods
• Descriptive
- Variation analysis – arithmetic mean and standard error (mean±SEM);
- Alternative analysis – evaluation of the relative share in (%).
• Parametric analysis
- Student's t-test - difference between two independent samples.
- univariate and multivariate regression analysis
• Non-parametric analysis:
- χ2 - Pearson's test
- Kruskal-Wallis criterion
- Fisher's exact test
- Kolmogorov-Smirnov test.
• Significance level of null hypothesis P=0.05, confidence interval 95%.
• Correlation analysis – Pearson's linear correlation coefficient (r).
• Data processing and analysis - SPSS v.19. The graphical presentation MS Excel for Windows.
Contingent
Study cohort consisted of 124 patients with a diagnosis of COPD and a control group of 162 individuals without lung disease. Persons studied are over 18 years of age, of different genders, of Bulgarian ethnic origin and with different family and social status.
| characteristic | men | women | ||||
| number | р % | Sp | number | р % | Sp | |
| residence | ||||||
| village | 14 | 19.18 | 4.61 | 15 | 20.55 | 4.73 |
| city | 41 | 56.16 | 5.81 | 41 | 56.16 | 5.81 |
| regional city | 18 | 24.66 | 5.04 | 17 | 23.29 | 4.95 |
| total | 73 | 100 | 73 | 100 | ||
| Marital status | ||||||
| Family | 48 | 65.75 | 5,55 | 38 | 52.05 | 5.85 |
| unmarried | 14 | 19.18 | 4,61 | 9 | 12.33 | 3.85 |
| A widower | 11 | 15.07 | 4,19 | 26 | 35.62 | 5.60 |
| total | 73 | 100 | 73 | 100 | ||
| Education | ||||||
| High | 22 | 30.10 | 5.37 | 24 | 32.88 | 5.50 |
| Average | 44 | 60.30 | 5.73 | 38 | 52.05 | 5.85 |
| Mainly | 7 | 9.60 | 3.45 | 11 | 15.07 | 4.19 |
| total | 73 | 100 | 73 | 100 | ||
| Employment | ||||||
| working | 28 | 38.40 | 5.69 | 24 | 32.88 | 5.50 |
| unemployed | 6 | 8.20 | 3.21 | 5 | 6.85 | 2.96 |
| pensioner | 39 | 53.40 | 5.84 | 44 | 60.27 | 5.73 |
| total | 73 | 100 | 73 | 100 | ||
Table 1: Distribution of patients with COPD by socio-demographic indicators
Distribution by gender and age of patients with COPD: men 73, average age 60.17±2.48 years; women 73, mean age 62.27±2.78 years. Relative share is highest in patients living in a city: men (56.16%) women (56.16%); family: men (65.75%) women (52.05%). By education, highest relative share is with secondary education: men (60.30%) women (52.05%), pensioners: men (53.40%) women (60.27%).
| diagnoses | is sick | 18 - 39 years | 40 - 59 years | 60 years + | total | ||||
| number | % | number | % | number | % | number | % | ||
Mild COPD
| No | 4 | 100 | 49 | 89.1 | 79 | 90.8 | 132 | 90.4 |
| Yes | 0 | 0 | 6 | 10.9 | 8 | 9.2 | 14 | 9.6 | |
Moderate COPD | No | 4 | 100 | 48 | 87.3 | 74 | 85.1 | 126 | 86.3 |
| Yes | 0 | 0 | 7 | 12.7 | 13 | 14.9 | 20 | 13.7 | |
| Severe COPD | No | 4 | 100 | 50 | 90.9 | 60 | 69 | 114 | 78.1 |
| Yes | 0 | 0 | 5 | 9.1 | 27 | 31 | 32 | 21.9 | |
| Very severe COPD | No | 2 | 50 | 33 | 60 | 48 | 55.2 | 83 | 56.8 |
| Yes | 2 | 50 | 22 | 40 | 39 | 44.8 | 63 | 43.2 | |
Table 2: Distribution of patients by diagnosis and age
A relationship was established between age of severe COPD (χ2=10.60, df=2, P<0 df=2,>0.05).
| characteristic | men | women | ||||
| number | р % | Sp | number | р % | Sp | |
| Residence | ||||||
| village | 5 | 6.94 | 3.00 | 6 | 6.57 | 2.63 |
| City | 49 | 68.06 | 5.49 | 57 | 63.33 | 5.08 |
| Regional city | 18 | 25.00 | 5.10 | 27 | 30.00 | 4.83 |
| total | 72 | 100 | 90 | 100 | ||
| Marital status | ||||||
| family | 42 | 58.33 | 5.81 | 62 | 68.89 | 4.88 |
| unmarried | 25 | 34.72 | 5.61 | 27 | 3.00 | 4.83 |
| widower | 5 | 6.94 | 3.00 | 1 | 1.11 | 1.10 |
| total | 72 | 100 | 90 | 100 | ||
| Education | ||||||
| high | 41 | 56.94 | 5.84 | 81 | 90.00 | 3.16 |
| average | 30 | 41.67 | 5.81 | 9 | 10.00 | 3.16 |
| basically | 1 | 1.39 | 1.38 | 0 | 0.00 | 0.00 |
| total | 72 | 100 | 90 | 100 | ||
| Employment | ||||||
| working | 59 | 81.94 | 4.53 | 82 | 91.11 | 3.00 |
| unemployed | 3 | 4.17 | 2.35 | 6 | 6.67 | 2.63 |
| pensioner | 10 | 13.89 | 4.08 | 2 | 2.22 | 1.55 |
| total | 72 | 100 | 90 | 100 | ||
Table 3: Distribution of control group by socio-demographic indicators
Highest is relative share of men (68.06%), and women (63.33%) living in a city. By marital status, relative share of married women is highest (68.89%). Family men are (58.33%). In terms of education, relative share of women with higher education (90%) is higher, for men it is (56.94%). Among persons from the control group, there are most workers: men (81.94%), women (91.11%).
Self-assessment of physical activity
Patients define their physical activity as "High" men (4.1%) and women (9.6%) "Average" rating men (50.7%) and women (35.6%). "Low" activity in men (45.2%) and women (54.8%). There is a relationship between education and self-assessment of physical activity (χ2=20. 71, df=4, p=0.001), as well as between employment and physical activity (χ2=20.26, df=4, p=0.001).
In the control group, physical activity is "High" in men (16.7%) and women (23.3%). "Average" activity in men (65.3%) and women (65.6%). "Low" is for men (18.1%) and women (11.1%).
A better self-assessment of physical activity was found in men and women of the control group. Age is a factor for physical activity (χ2=10.72, df=4, p=0.01).
There is a statistically significant difference for physical activity between patients and controls (χ2=48.58, df=2, p=0.001).

Figure 1. Comparative characteristics of men patients and controls on question: "How do you rate your physical activity in last month?"
Figure 2. Comparative characteristics of women patients and controls on question: "How do you rate your physical activity in last month?"
Self-reported physical activity was low for half of the subjects in patient group. A statistically significant difference was found for physical activity between patients and controls.
Smoking
Smoking patients were men (28.8%), and women (16.4%). Relative share of smokers 40-59 years (32.7%). There is an association between smoking and age (χ2=8.95, df=2, p=0.01). Relative share of smokers living in city (43.4%) is largest, and smallest in the villages (36.4%).
In the control group, smokers were men (47.8%), women (52.2%). Relative share of smokers 40-59 age (42.7%). There was no statistically significant difference between men smokers two studied groups: patients and controls (U=1.4, P>0.05)
| patients | smokers | non-smokers | total | |||
| gender | number | % | number | % | number | % |
| Men | 21 | 28.8 | 52 | 71.2 | 73 | 100 |
| Women | 12 | 16.4 | 61 | 83.6 | 73 | 100 |
| age | ||||||
| 18-39 years | 2 | 50 | 2 | 50 | 4 | 100 |
| 40-59 years | 18 | 32.7 | 37 | 67.3 | 55 | 100 |
| 60 years + | 12 | 13.8 | 75 | 86.2 | 87 | 100 |
| place of residence | ||||||
| city | 22 | 26.8 | 60 | 73.2 | 82 | 100 |
| village | 4 | 13.8 | 25 | 86.2 | 29 | 100 |
| Regional city | 6 | 17.1 | 29 | 82.9 | 35 | 100 |
| controls | ||||||
| gender | ||||||
| men | 33 | 47.8 | 39 | 41.9 | 72 | 100 |
| women | 36 | 52.2 | 54 | 58.1 | 90 | 100 |
| age | ||||||
| 18-39 years | 24 | 39.3 | 37 | 60.7 | 61 | 100 |
| 40-59 years | 35 | 42.7 | 47 | 57.3 | 82 | 100 |
| 60 years + | 10 | 52.6 | 9 | 47.4 | 19 | 100 |
| place of residence | ||||||
| City | 46 | 43.4 | 60 | 56.6 | 106 | 100 |
| village | 4 | 36.4 | 7 | 63.6 | 11 | 100 |
| Regional city | 19 | 42.2 | 26 | 57.8 | 45 | 100 |
Table 4. Distribution of smoking, sex, age and place of residence
Smokers predominated in control group (42.6%) compared to patient group (22.6%). With increasing age, a decrease in the relative share of smokers is observed.
A study of personality anxiety
Questionnaire (STAI) is an instrument for measuring anxiety, adapted from P. Paspalanov and D. Shchetinsky, 1989: as a personality trait and as a state. Values of personal anxiety are: men – 43.7; SD=9.1; women – 48.8; SD=9.6. Individuals with a mean score above these values exhibited personal anxiety. A non-parametric Kolmogorov-Smirnov test was performed for normal distribution of cases in the samples. Distribution is normal (P>0.05).
| patients and controls | |||||
| gender | mean | SD | SEM | t | p-value |
| Men patients | 44.41 | 9.16 | 1.07 | 4.50 | p<0> |
| Men controls | 43.08 | 7.13 | 0.66 | ||
| Women patients | 47.16 | 8.86 | 1.03 | 4.49 | p<0> |
| Women controls | 41.16 | 5.62 | 0.75 | ||
Table 5. Comparative anxiety parameters between patients and controls
Comparisons of mean values for anxiety in patients and controls were performed with Student-Fisher test and a significance level of P=0.05. Mean value for patients was (45.78) and for controls (42.1) (t=4.14, p<0 t=4.5, t=4.49, t=2.02, t=1.86,>0.05). Results of a group of patients showed presence of anxiety (49.3%). Of them men (53.42%), women (45.20%). In the control group (21.6%) respondents had anxiety. Of them men (23.6%), women (20.0%).
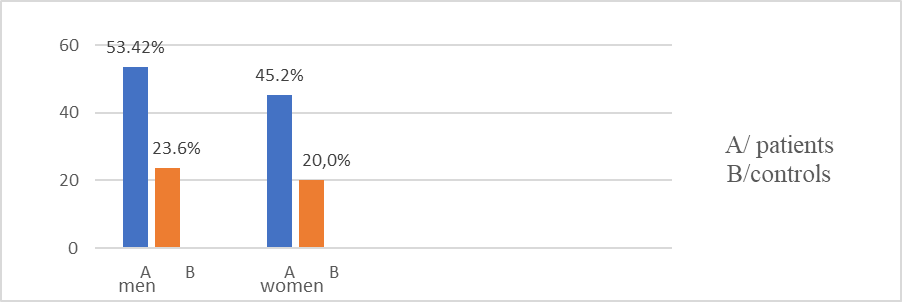
Figure 3. Distribution of patients and controls by gender and anxiety
Anxiety is present in patients living in small settlements (60%); single (56.5%); with primary education (72.2%); and pensioners (62.7%). There is an association between anxiety and place of residence (χ2=8.95, df=2, p=0.001). A relationship was established between anxiety and education (χ2=9.53, df=2, p=0.009); anxiety and employment (χ2=14.68, df=2, p=0.001); anxiety and age (χ2=9.55, df=2, p=0.008).
From an anxiety test above norm was in control group 40-59 years (20.7%) family (25.1%) with higher education (23.1%) working (22.7%) in cities (24.5%). There is no relationship between anxiety and demographics (P>0.05)
| anxiety | patients | controls | ||||
| number | р % | χ2 p-value | number | р % | χ2 p-value | |
| age | ||||||
| 18-39 years | 1 | 1.4 | χ2=9.55 p=0.008 | 11 | 18 | NS |
| 40-59 years | 19 | 26.4 | 17 | 20.7 | ||
| 60 years + | 52 | 72.2 | 7 | 36.8 | ||
| Residence | ||||||
| village | 20 | 27.8 | χ2=8.95 p=0.01 | 2 | 18.2 | NS |
| City | 41 | 56.9 | 26 | 24.5 | ||
| Regional city | 11 | 15.3 | 7 | 15.6 | ||
| Education | NS | |||||
| high | 15 | 20.8 | χ2=9.53 p=0.09 | 28 | 23 | |
| average | 44 | 61.1 | 7 | 17.9 | ||
| basically | 13 | 18.1 | 0 | 0 | ||
| Marital status | NS | |||||
| Family | 39 | 54.2 | NS | 24 | 23.1 | |
| unmarried | 13 | 18.1 | 11 | 21.2 | ||
| widower | 20 | 27.8 | 0 | 0 | ||
| Employment | ||||||
| Working | 15 | 20.8 | χ2= 14.68 p=0.001 | 32 | 22.7 | NS |
| unemployed | 5 | 6.9 | 0 | 0 | ||
| pensioner | 52 | 72.2 | 3 | 25 | ||
Table 6. Distribution of Patients and Controls by Demographic Characteristics and Anxiety
Patients with COPD and anxiety (54.7%). Of them, anxiety (97.2%); with mild COPD – (11.1%); with moderate COPD – (15.3%); with severe COPD (29.2%); with very severe COPD – (41.7%). There is a relationship between anxiety and hypertensive disease (χ2=7.6, df=1, p=0.006); between anxiety and severe COPD (χ2=4.4, df=1, p=0.03). There is no association between anxiety and other forms of COPD (P>0.05).
A study of personality traits by type D
The "D" Scale-14 questionnaire is a modern methodology for determining characteristics of the D-type personality (J. Denollet, A. Shiffer, V. Spek, 2010). Results of the study of two groups provide a basis for comparison and interpretation of an association between personality traits and COPD.
| patients | controls | |
| D personality dimensions | KS - test, p-value | KS - test, p-value |
| social inhibition | 0.91; p>0.05 | 1.23; p>0.05 |
| negative affectivity | 0.67; p>0.05 | 1.48; p>0.05 |
Table 7: Results of a non-parametric test for normal sampling frequency distribution
A parametric test of working hypothesis was performed with a significance level of P=0.05. A Student-Fisher t-test was used to compare mean values of D Personality Questionnaire responses of patients and controls. There was a statistically significant difference in mean values between patients and controls: patients (mean 23.05, SD 9.83); controls (mean 17.45, SD 6.8) (t=5.39, p<0>
A statistically significant difference was found in mean values for "social inhibition" dimension between patients (mean 10.14, SD 5.4) and controls (mean 7.44, SD 4.01) (t=4.27; p<0>
➢ A statistically significant difference was found in mean values of "negative affectivity" dimension between patients (mean 12.77, SD 6.7) and controls (mean 10.54, SD 4.4) (t=3.4; p<0>
From the personality type D questionnaire, average values of patients on dimensions "social inhibition" and "negative affectivity" were above 10, indicating manifestation of personality type D characteristics (57.5%). In the control group, average value of "social inhibition" dimension is below 10, which shows that they do not have a clearly defined type D personality (31.5%).
| patients | controls | ||||
| D personality dimensions | Mean | SD | mean | SD | t-test,p-value |
| social inhibition | 10.14 | 5.4 | 7.44 | 4.01 | t=4.27; p<0> |
| negative affectivity | 12.77 | 6.7 | 1.54 | 4.4 | t=3.4; p<0> |
| common to both dimensio | 23.05 | 9.83 | 17.45 | 6.8 | t=5.39; p<0> |
Table 8: Comparative parameters of patients and controls for the dimension D personality type
In the group of patients, a correlation was found between gender and "social inhibition" dimension (χ2=5.6, df=1, p=0.03). There is a relationship between education and "negative affectivity" dimension (χ2=6.7, df=1, p=0.03). Employment and marital status have a relationship with individuals exhibiting "negative affectivity" (χ2=7.22, df=2, p=0.02); (χ2=14.29, df=2, p=0.001). In the control group, there is an association between "negative affectivity" dimension and marital status (χ2=6.76, df=2, p=0.03)
For "negative affectivity" dimension, a value above 10 was found in (62.3%) patients, women (65.6%); men (58.8%). Relative share of patients is greatest among persons over 60 years (60%); living in villages (75.9%); with primary education (88.9%); single (81.1%); and pensioners (74.4%).
| personality type D | patients | controls | patients | controls | ||||||||
| Social inhibition | Negative affectivity | |||||||||||
N
| р %
| χ2; p-value | N
| р %
| χ2; p-value | N | р %
| χ2; p-value | N | р %
| χ2; p-value | |
| gender | ||||||||||||
| Men | 32 | 43.8 | χ2=5.6, p=0.03 | 21 | 29.2 | NS | 43 | 58.9 | NS | 33 | 45.8 | NS |
| Women | 45 | 61.5 | 17 | 18.9 | 48 | 65.6 | 43 | 47.8 | ||||
| age | ||||||||||||
| 18-39 years | 1 | 25.0 | NS | 9 | 14.8 | NS | 1 | 25.0 | NS | 29 | 47.5 | NS |
| 40-59 years | 28 | 50.9 | 24 | 29.1 | 30 | 54.5 | 39 | 47.6 | ||||
| 60 years + | 48 | 55.2 | 5 | 36.3 | 60 | 69.0 | 8 | 42.1 | ||||
| Residence | ||||||||||||
| village | 19 | 65.5 | NS | 5 | 45.5 | NS | 22 | 75.9 | NS | 8 | 72.2 | NS |
| city | 42 | 51.2 | 24 | 22.6 | 49 | 59.8 | 50 | 47.2 | ||||
| Regional city | 16 | 45.7 | 9 | 20.0 | 20 | 57.1 | 18 | 40.0 | ||||
| Education | ||||||||||||
| high | 24 | 52.2 | NS | 26 | 21.3 | NS | 25 | 54.3 | χ2=6.7, p=0.03 | 56 | 45.9 | NS |
| average | 42 | 51.2 | 11 | 28.2 | 50 | 61.0 | 20 | 51.3 | ||||
| basically | 16 | 45.7 | 1 | 100 | 16 | 88.9 | 0 | |||||
| Marital status | ||||||||||||
| family | 44 | 51.2 | NS | 24 | 23.1 | χ2=6.7, p=0.03 | 47 | 54.7 | χ2=7.72, p=0.02 | 47 | 45.2 | NS |
| unmarried | 12 | 52.2 | 10 | 19.2 | 14 | 60.9 | 26 | 50.0 | ||||
| widower | 21 | 56.8 | 4 | 66.7 | 30 | 81.1 | 3 | 50.0 | ||||
| Employment | ||||||||||||
| working | 25 | 48.1 | NS | 33 | 23.4 | NS | 22 | 42.3 | χ2=14.29, p=0.001 | 66 | 46.8 | NS |
| unemployed | 6 | 45.5 | 1 | 11.1 | 7 | 63.3 | 5 | 55.6 | ||||
| pensioner | 46 | 55.4 | 4 | 33.3 | 62 | 74.4 | 5 | 41.7 | ||||
Table 9. Distribution of Patients and Controls by Demographics and Personality Type D Characteristics
From control group, average value is over 10 for dimension "negative affectivity" in women (47.8%); men (45.8%); 40-59 years (47.6%); living in village (72.2%); with secondary education (51.3%); single (50%); and pensioners (55.6%).
Dimension "social inhibition" was evident in female patients (61.6%).Highest relative share is over 60 years (55.2%); living in villages (65.5%); single (56.8%), pensioners (55.4%). In the control group, relative share of "social inhibition" dimension is smaller (23.5%). Women are (18.9%); and men (29.1%). Largest relative share is people over 60 (36.3%); living in villages (45.5%); single (66.6%); and pensioners (33.3%).
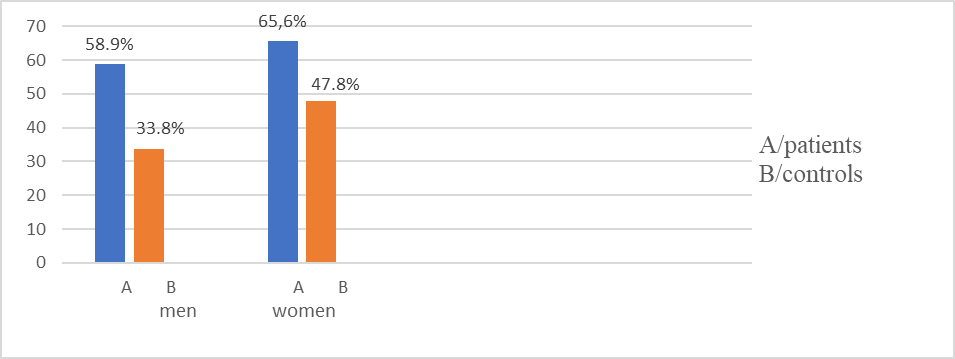
Figure 4. Comparative parameters for “negative affectivity“ dimension for patients and controls by gender
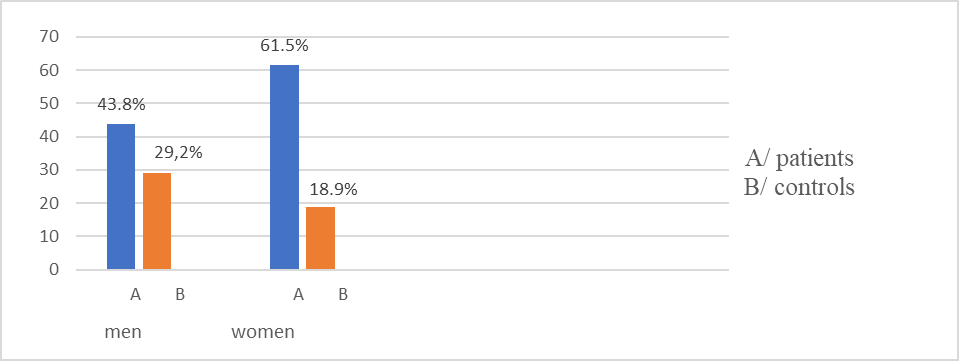
Figure 5. Comparative parameters for "social inhibition" dimension for patients and controls by gender
In the group of patients with anxiety and personality type D are (42.55%) . With anxiety and dimension "social inhibition" are (59.72%). There is a relationship between anxiety and "social inhibition" (χ2=15.90, df=1, p=0.001). Patients with anxiety and dimension "negative affectivity" (86.11%). There is a relationship between anxiety and "negative affectivity" (χ2=34.21, df=1, p=0.001). Patients with personality type D have higher levels of anxiety, more pronounced in women. Values for dimensions "social inhibition" and "negative affectivity" are (65.6%).
In the control group with anxiety and type D personality traits were (34.3%). With "anxiety" and "social inhibition" (22.9%); and with "negative affectivity" (45.7%). There is no relationship between anxiety and dimensions "social inhibition" and "negative affectivity" (P>0.05). of control group, they exhibited characteristics of "social inhibition" (23.5%).
Social adaptability
Patient group and control group answered questions on social life and coping with personal and professional commitments. Assessment is carried out on a 4-point Likert scale: weak - 1 point; low - 2 points; medium – 3 points; high - 4 points. A parametric test of working hypothesis was performed with t-criterion, at a significance level of P=0.05.
1. Question: To what extent are you coping with work and/or family commitments?
Patients showed a "high" level of coping in men (13.7%), and women (9.6%). An "average" level of coping was reported for men (13.7%), and women (20.5%) and a "low" level of coping for men (43.8%), and women (39.7%)."weakly" self-assessment of professional and family commitment for men (28.8%), and women (30.1%)
In the control group, men (41.7%), and women (47.8%) showed a "high" level of coping, a "average" level in men (50.0%), and women (48.9%) , "low" level in men (6.9%), and women (2.2%), "weakly" level men (1.4%), women (1.1%).
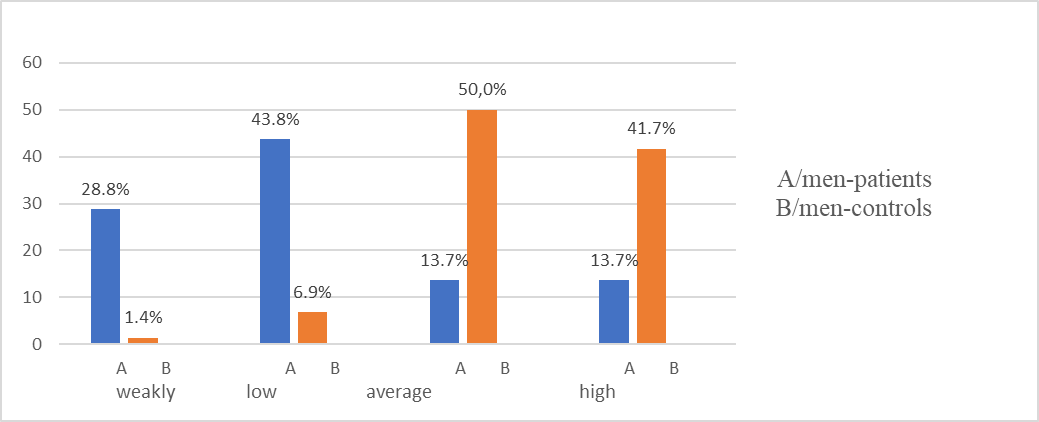
Figure 6. Comparative characteristics between male patients and controls on question: "To what extent do you cope with professional and/or family commitments
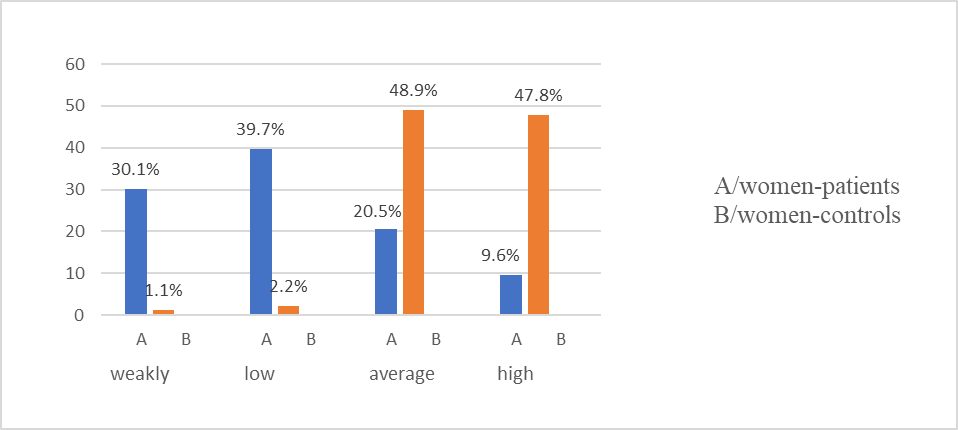
Figure 7. Comparative characteristics between female patients and controls on question: "To what extent do you cope with professional and/or family commitments?"
No relationship was found between coping abilities and demographic characteristics (P>0.05). Mean response values for patients 2.89±0.96 and control group 3.38±0.63. There was a statistically significant difference in mean response values in patients and controls (t =5.19, P<0>
2.Question: How often do you communicate with your family members?
Patients communicate with family "very often" men (1.4%), and women (4.10%), "often" communication men (8.20%), and women (11%),
"sometimes" men (57.50%), and women (50.70%), "rarely" men (32.90%), and women (34.2%).
From the control group, men (27.8%) and women (41.1%) communicate with the family "very often", "often" men (59.7%), and women (54.40%), "sometimes" men (12.50%), and women (4.40%), "rarely" men (0%), and women (0%).
There was no correlation between communication with family and demographic characteristics of two groups (P>0.05).
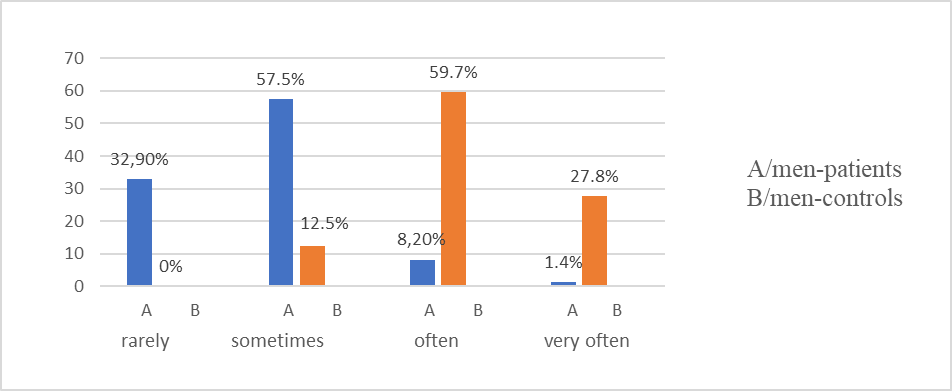
Figure 8. Comparative characteristics between male patients and controls on question: "How often do you communicate with your family members?"
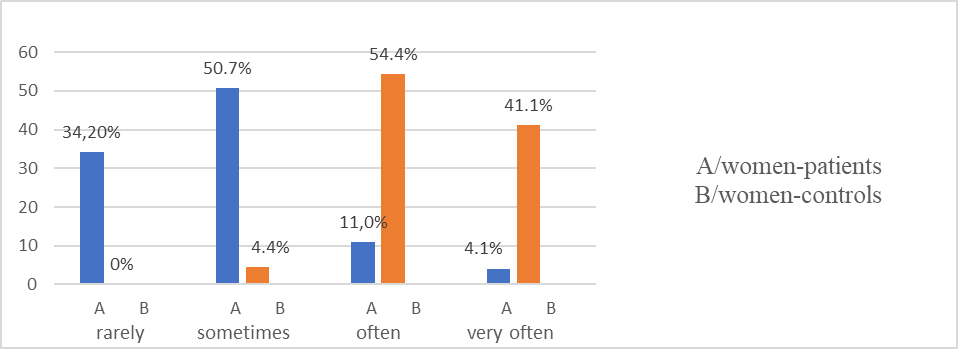
Figure 9. Comparative characteristics between female patients and controls on question: "How often do you communicate with your family members?"
3.Question: "How often do you communicate with friends, colleagues and acquaintances?"
From patients communication with friends and colleagues "Very often" men (0%)and women (1.4%). "Often" communication men (17.8%) and women (42.5%) "Sometimes" for communication with male friends and colleagues (67.1%), and women (34.2%). Communication is "rarely" for men (15.1%), and women (21.9%).
In the control group communication with colleagues and friends "Very often" men (25%), and women (30%), and women. "Often" men (52.8%), and women (58.9%) "Sometimes" men (22.2%), and women (11.1%). "Rarely" is communication for men (0%), and women (0%).
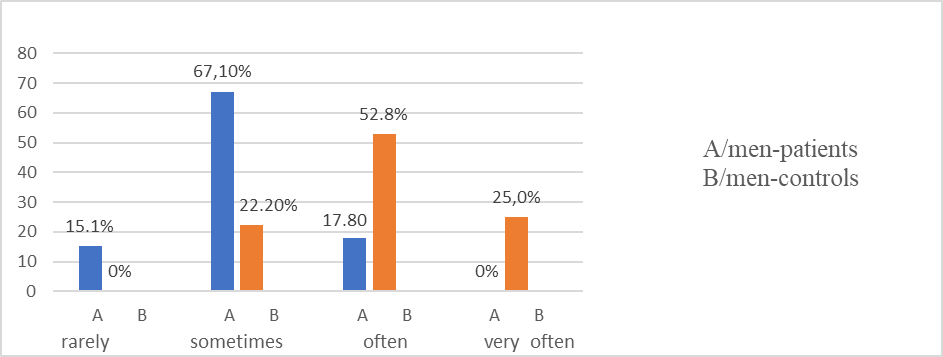
Figure 10. Comparative characteristics between male patients and controls on question: "How often do you communicate with friends, colleagues and acquaintances?"

Figure 11. Comparative characteristics between female patients and controls on question: "How often do you communicate with friends, colleagues and acquaintances?"
There is a relationship between the frequency of communication with acquaintances, colleagues and friends and education (χ2=13.31, df=3, p=0.001), and with gender (χ2=17.07, df=3, p=0.001). A correlation was found between age (χ2=18.84, df=4, p=0.001); education (χ2=12.58, df=4, p=0.01); employment (χ2=14.98, df=4, p=0.005).
4.Question: "Are you able to organize your life according to your needs?"
Patients who cope "Very good " with organizing their lives are men (6.8%) and women (11.0%). Men (32.9%) and women (41.1%) have "good" organization of everyday life, "Satisfactory" men (52.1%) and women (42.5%). " Bad " self-assessment for coping men (8.2%) and women (5.5 %).
In the control group "Very good" men (23.3%) and women (19.2%), "Good" organization men (37.0%) and women (42.0%). Men (35.6%) and women (32.0%) gave a "satisfactory" rating, " Bad " organization men (4.4%) and women (6.8%).
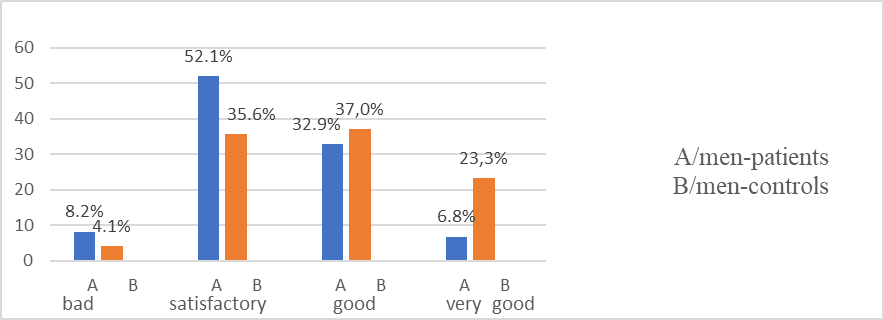
Figure 12. Comparative characteristics between male patients and controls on question: "Are you able to organize your life according to your needs?"
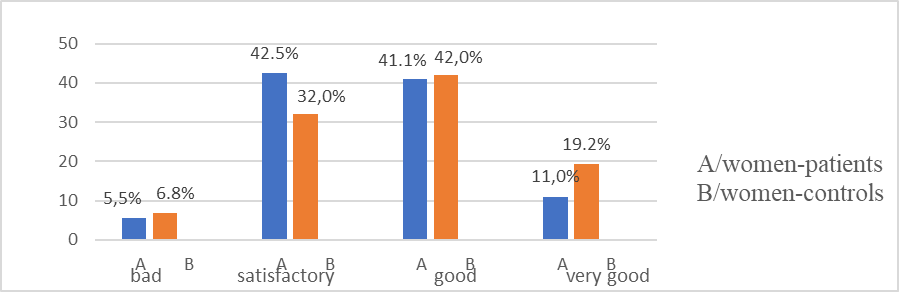
Figure 13. Comparative characteristics between female patients and controls on question: "Are you able to organize your life according to your needs?"
There is no dependence in distribution of patients and controls according to demographic indicators and organization of life (P>0.05).
Mean value of the responses in the patients was 2.52±0.71 and control group 2.96±0.62. There is a statistically significant difference (t=6.10, P<0>
5.Question "How do you define your life in last month?
Patients give "Very good" self-assessment of life men (23.3%) and women (19.2%). "Good" is t assessment of life for men (37.0%) and women (36.5%). "Satisfactory" for men (35.6%) and women (37.5%). "Bad" is the rating for men (4.1%) and women (6.8%).
In the control group, self-assessment of life is "Very good" men (23.4%) and women (23.3%), "Good" assessment in men (44.4%) and women (56.7%). Men (32.3%) and women (17.8%) indicated a "satisfactory" rating. "Bad" evaluation of life men (0%) and women (2.2%).
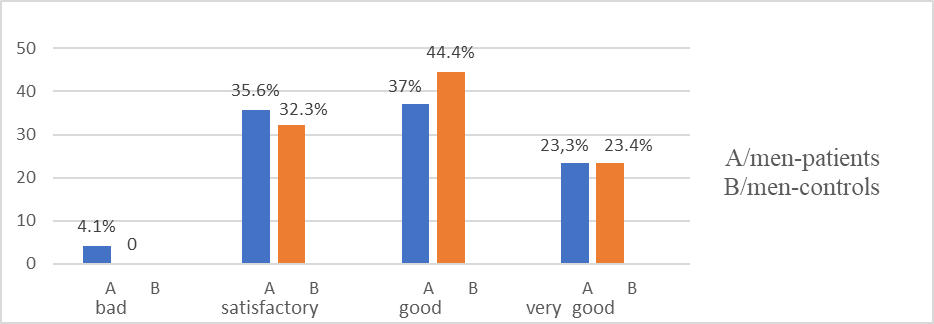
Figure 14. Comparative characteristics between male patients and controls on question:
How would you rate your life in last month?
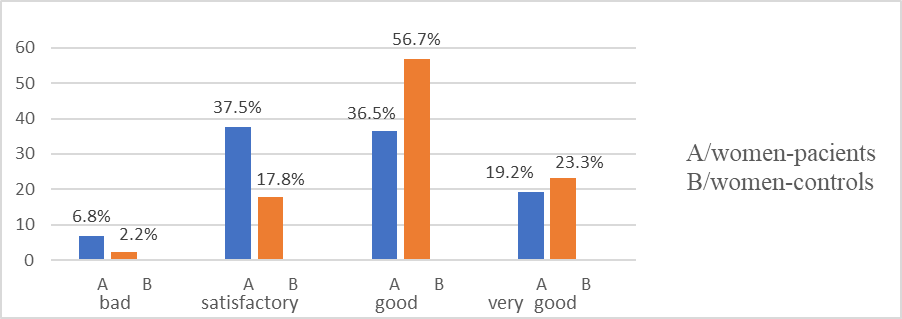
Figure 15. Comparative characteristics between female patients and controls on question: How would you rate your life in last month?"
There was no association in distribution of patients and controls by demographic indicators and self-rated quality of life (P>0.05). Mean value for patients was 2.26±0.85, for the control group 2.96±0.79. There is a statistically significant difference (t=8.14, P<0>
6.Question: Are you trying to make new social connections?
Patients for seeking new social contacts indicate "very often" men (8.2%) and women (6.8%). Men (27.4%) create new contacts "often" women (37.0%). Men (57.5%), and women (47.9%) look for new contacts "sometimes".
In the "very often" control group, men (14.8%), and women (22.2%) for making new contacts. "Often" creation of new acquaintances is reported for men (52.8%) and women (71.1%). Аnswer "sometimes" was given by men (21.6%) and women (23.5%).
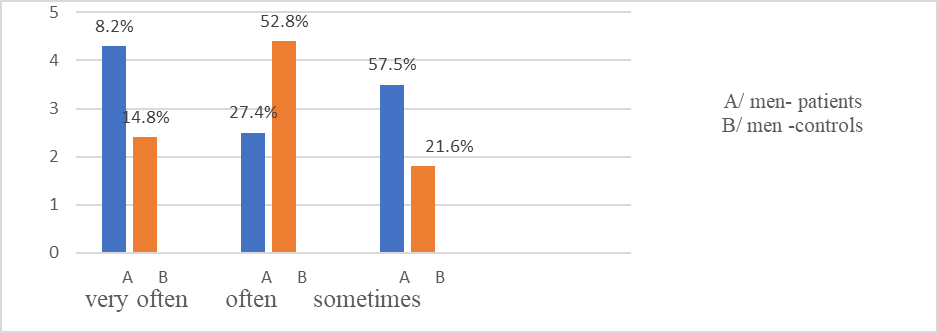
Figure 16: Comparative characteristics between female patients and controls on question: Do you try to make new social contacts?"
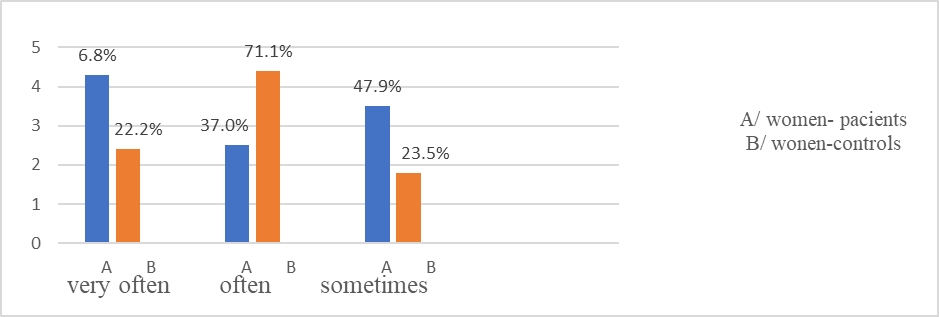
Figure 17: Comparative characteristics between female patients and controls on the question: Do you try to make new social contacts?"
Gender, age, marital status and place of residence are not factors for the realization of new social contacts in patients (P>0.05). Gender is a factor for creating new social contacts in controls (χ2=14.90, df=3, p=0.002).
Patients experience certain difficulties in creating new social contacts. Mean value of responses for patients 2.60±0.74 and control group 2.92±0.62. A parametric test was performed to compare means and there was a statistically significant difference (t-test 4.44, P<0>
Psychosocial factors, social engagement and living environment have a major impact on the quality of life of COPD patients. Anxiety has been found to be associated with some "social adjustment" problems in patients.
In patients, there is a relationship between anxiety and coping with professional and family commitments (χ2=27.21, df=3, p=0.001); communicating with friends and colleagues" (χ2=10.58, df=3, p=0.01); "organizing everyday life" (χ2=22.37, df=3, p=0.001) and "life evaluation in the last month" (χ2= 26.17 , df=3, p=0.001).
In the control group, anxiety was a factor for dealing with "family and professional activities" (χ2=11.43, df=3, p=0.01). The remaining social adjustment questions were not related to anxiety (P>0.05).
There is a relationship between anxiety and certain demographic characteristics. People who live in cities, the unemployed, and the retired have symptoms of anxiety. Anxiety negatively affects patients' social life,
coping with professional and family commitments, social communication, organization of daily life and self-assessment of health.
Health-Related Quality of Life Survey
Through the EQ-5D questionnaire, domains related to physical functioning, coping with daily activities, home and personal care, disease symptoms and psycho-emotional problems are investigated.
➢ Among the patients, there are problems with "mobility" in men (43.9%) and women (56.1%). Difficulties in mobility are present at 60+ years (75.9%) and 40-59 years (56.4%). Difficulties were found for those living in villages (82.2%), cities (64.4%), non-family (75.7%), family (56.1%); with secondary education (69.5%) pensioners (80.7%). There is a correlation between mobility and gender (χ2=4.46, df=2, p=0.03). There is a correlation between "mobility" and age (χ2=9.11, df=2, p=0.01); education (χ2=7.47, df=2, p=0.02) and employment (χ2=14.29, df=2, p=0.001).
In the control group, difficulties in "mobility" were experienced by men (19.4%), women (11.1%). The relative share of pensioners (41.7%), with secondary education (17.9%), unmarried (33.3%), living in a regional town (17.8%) is the largest. There is a relationship between mobility and age (χ2=16.7, df=2, p=0.05), with employment (χ2=7.42, df=2, p=0.03).
A statistically significant difference was found in relative proportions for mobility dimension between patients and controls: males (U=3.05; p<0 U=5.58;>
Figure 18. Relative share of patients with problems in QZS by age groups
Men (32.9%) and women (38.4%) patients have difficulties in "self-care" dimension. Over 60 years of age have difficulties (46%), living in villages (51.7%), with primary education (66.7%). Relative share of patients with self-care problems is largest among unmarried patients (48.6%) pensioners (50.6%). There is a relationship between self-care and age (χ2=10.85, df=1, p=0.004), with education (χ2=14.64, df=2, p=0.001) and with employment (χ2=21.27, df=2, p= 0.001). In the control group, there were difficulties in self-care in 1 man and 2 women, married, working and with secondary and higher education
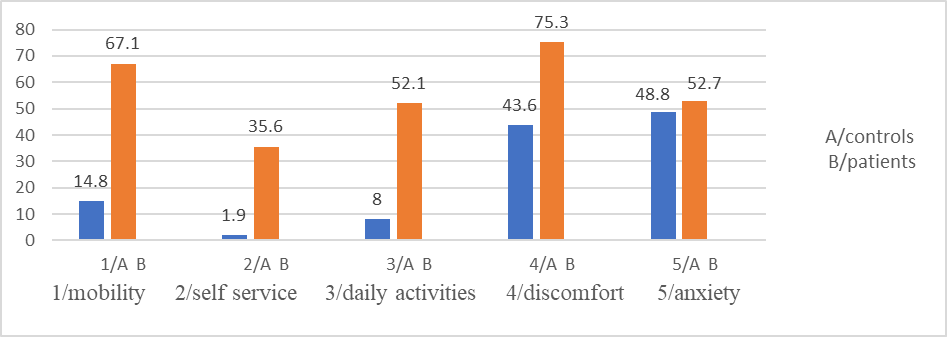
Figure 19. Distribution of patients and controls with problems by EQ-5D questionnaire dimensions
Difficulties in performing "daily activities" patients men (45.2%) and women (58.9%). Relative share of problems is greatest in patients over 60 age (65.5%); living in villages (58.7%); single (67.6%); with primary education (72.2%) pensioners (73.5%). There is an association between field "usual activities" and age (χ2=17.41, df=2, p=0.001), education (χ2=11.28, df=2, p=0.004) employment (χ2=35.48, df=2, p<0 df=2, p=0.005), df=2, p=0.003) xss=removed p=0.03).>
Рatients men (72.6%) , women (78.1%) had difficulties in "discomfort" dimension.Largest relative share is over age of 60 with difficulties (83.9%), of patients living in villages (93.1%) single (78.4%). High relative share is among persons with primary education (88.9%) pensioners (85.5%). There is a relationship between "discomfort" domain and age (χ2=11.78, df=2, p=0.003), place of residence (χ2=6.15, df=2, p=0.04), education (χ2=6.20, df=2, p=0.04) employment (χ2=13.61, df=2, p=0.001).
Difficulties in "discomfort" dimension were found men (56.9%) women (48.9%) controls. Highest relative share is found in: over 60 age (78.9%); in villages (63.6%), without partner (66.7%), with secondary education (53.8%) pensioners (91.7%). Relationship was established between "discomfort" and employment (χ2=8.13, df=2, p=0.01), with age (χ2=6.05, df=2, p=0.04). Statistically significant difference was found in relative share of "pain/discomfort" dimension between female patients and controls (U=3.13; p<0 U=1.59;>
Dimension for assessment of "anxiety". Symptoms of anxiety are present in men (57.5%), women (63%). Most difficulties are over 60 age (62.1%). Highest relative share of patients in villages (86.2%), non-family (70.3%), pensioners (68.7%) with primary education (88.9%). There is a relationship between dimension and age (χ2=6.24, df=2, p=0.04), place of residence (χ2=13.74, df=2, p=0.005) marital status (χ2=10.38%, df=2, p=0.006 ).
Controls, problems in " anxiety " dimension in men (56.9%) women (48.9%). Relative share is largest over 60 age (68.4%), in villages (54.5%), unmarried (83.3%), with secondary education (56.4%), pensioners (75%). Association was found between dimension and age (χ2=6.36, df=2, p=0.04). There was no statistically significant difference in relative proportions for "anxiety/depression" dimension between patients and controls: men (U=0.30; P˃0.05), women (U=1.75; P˃0.05)
| patients | controls | ||||
| EQ-5D dimensions | age | number% | χ2, р-value | number% | χ2, р-value |
mobility
| 18-39 years | 1.25 | χ2=9.11, p=0.01 | 4/6.6 | χ2=10.67, p=0.005 |
| 40-59 years | 31/56.4 | 13/15.9 | |||
| 60 years + | 66/75.9 | 7/36.8 | |||
| self service | 18.39 years | χ2=10.85, p=0.004 | |||
| 40-59 years | 12/21.8 | 3.37 | |||
| 60 years + | 40/46 | ||||
| usual activities | 18-39 years | χ2=17.41, p=0.001 | 2/3.3 | χ2=10.53, p=0.05 | |
| 40-59 years | 19/34.5 | 6/7.3 | |||
| 60 years + | 57/65.5 | 5/26.3 | |||
discomfort | 18-39 years | 1.25 | χ2=11.78, p=0.003 | 30/49.2 | χ2=6.05, p=0.04 |
| 40-59 years | 36/65.5 | 40/48.4 | |||
| 60 years + | 73/83.9 | 15/78.9 | |||
| anxiety | 18-39 years | χ2=6.24, p=0.04 | 23/27.7 | ||
| 40-59 years | 34/61.8 | 43/52.4 | |||
| 60 years + | 54/62.1 | 13/68.4 | |||
Table 10. Distribution of Patients and Controls by Age and Difficulty in Health-Related Quality of Life Dimensions
Relative share of patients with difficulties in spheres of quality of life is largest among pensioners, over 60 age, those living in villages, with primary education and unmarried. Control group, relative proportion with quality of life problems was lower.
Health assessment by visual analogue scale (VAS)
Mean value of self-rated health, on a scale of 0 to 100 was (52.74, SEM 1.69) points for patients and (78.56, SEM 0.96) points for control group. Statistically significant difference was found in mean values between patients and controls (t=13.5, p=0.001). There was a statistically significant difference between male patients and controls (t=7.7, p<0 t=10.82,>0.05).
| Health assessment | Mean | SD | Mean | SD | t-test, p-value |
| men | 53.97 | 20.05 | 75.03 | 11.95 | 7.7, p<0> |
| women | 51.51 | 21.06 | 81.38 | 11.77 | 10.82,p<0> |
Table 11. Comparative health assessment parameters by gender in patients and controls, by VA
Average values for health status of two age groups differ. As age increases, health assessment decreases in patients. Controls, health score was higher in all age groups, decreasing more smoothly with age. There is a statistically significant difference between health score and age of patients (Kruskal Wallis =22.72. df=5,p=0.001) 0.001)
| patients | controls | |||||
| age | mean | SD | Std.Error | mean | SD | Std.Error |
| 18-39 years | 70.06 | 18.25 | 9.12 | 80.25 | 11.94 | 1.53 |
| 40-59 years | 59.09 | 20.20 | 2.72 | 78.20 | 12.35 | 1.36 |
| 60 years + | 47.93 | 19.89 | 2.13 | 71.47 | 8.70 | 1.99 |
Table 12. Mean values of health assessment of patients and controls by age group, using VAS
As age increases, patients' assessment of health decreases. Pearson correlation coefficient was calculated (r= 0.369). Rank estimate of correlation coefficient indicates an inverse moderate relationship. For controls, relationship between two variables is inversely significant (r= 0.569).
Dependence between anxiety, type D personality and quality of life
➢ Patients with personal anxiety and problems in "mobility" dimension (61.2%). Controls, there were (16.7%). There is an association between anxiety and "mobility" dimension in patients (χ2=16.91, df=2, p=0.001).

Figure 20. Distribution of patients and controls with anxiety and difficulties in domains related to quality of life
Parametric test of working hypothesis was performed with a significance level of p=0.05. There is a statistically significant difference in relative proportions of patients and controls who exhibit anxiety and difficulties in physical activity (U=4.91; p<0>
There are (67.3%) patients with difficulties in field of "self-care" and showing anxiety. Controls with such problems are missing. There is an association between anxiety and self-care capabilities in patients (χ2=10.46, df=1, p=0.001).
There are (68.4%) patients who have difficulties in performing "daily activities" and with established anxiety. Controls with same problems, there were (15.4%). There is a relationship between anxiety and dimension "daily activities" in patients (χ2=23.15, df=1, p<0 U=4.68;>
There are (56.4%) patients with COPD showing anxiety and difficulties in "pain/discomfort" dimension (22.4%) were controls. Anxiety was a factor for presence of pain/discomfort in patients (χ2=8.86, df=1, p=0.002). There was a statistically significant difference in relative proportions of patients and controls with anxiety and pain/discomfort (U=5.2; p<0> χ2=16.91 p=0.001 χ2=10.46 p=0.001 χ2=23.15 p=0.001 χ2=8.86 p=0.002 anxiety patients anxiety controls Dimensions of QZ number % χ2, p-value number % χ2, p-value U- criterion mobility 60 (61.2%) 4 (16.7%) NS 4.91 Self service 35 (67.3%) 0 NS Daily activities 52 (68.4%) 2 (15.4%) NS 4.68 Discomfort 62 (56.4%) 19 (22.4%) NS 5.2
Table 13. Distribution of patients and controls with anxiety and problems in quality of life dimensions
Anxiety is a factor influencing the quality of life in patients with COPD. In them, a tendency to avoid physical activity, an increase in the severity of somatic symptoms and the emotional meaning of disease was found. Two dimensions of Type D personality and domains of the Quality of Life Questionnaire/QL/EQ-5D were analyzed. There is an association between patients exhibiting Type D personality traits and having difficulties in quality of life dimensions.
| Type D personality | ||
| EQ-5D - dimensions | Negative affectivity | Social isolation |
| Physical activity | χ2=13.0 df=1 p=0.001 | χ2=20.44 df=1 p=0.001 |
| Self service | χ2=7.32 df=1 p=0.007 | χ2=3.76 df=1 p=0.052 |
| Daily activities | χ2=21.71 df=1 p=0.001 | χ2=16.66 df=1 p=0.001 |
| Discomfort | χ2=11.18 df=1 p=0.001 | χ2=8.51 df=1 p=0.003 |
Table 14. Dependence between dimensions of type D personality and QOL in patients with COPD
Symptoms of patients with COPD have a negative impact on the quality of life. Patients show difficulties in physical activity. Reduced physical activity has a negative impact on self-care, daily activities, and self-assessment of health, prevailing among single people, in small settlements and with lower education. Combination of anxiety and D personality traits is associated with impaired quality of life and lower self-rated health. Compared to control group, they had fewer difficulties in the investigated areas of quality of life. No relationship was found between the domains of quality of life and the two dimensions of type D personality in control group (p>0.05).
When examining relationship between anxiety, type D personality and patients health assessment, established odds ratio showed that patients with type D personality had a 2.94 times greater risk of disease progression (OR 2.94 (95% CI) 1.84-4.71, P<0> factors Beta B±SE t P OR 95%CI P anxiety -0.523 0.123±0.166 -7.357 0.000 3.530 2.151; 5.793 0.000 personality type D -0.184 0.375±0.167 -2.246 0.026 2.948 1.848; 4.701 0.000 negative affectivity -0.463 0.438±0.229 -6.267 0.000 1.872 1.187; 2.951 0.006 social inhibition -0.259 0.988±0.307 -3.220 0.002 3.641 2.236; 5.292 0.000
Table 15. One-factor regression models for the influence of anxiety and type D personality
Psychosocial factors were analyzed by multivariate regression analysis. Reduced assessment of quality of life and health is due to influence of personality type D and personality anxiety (R²=0.647, P<0 R²=0.511,>
✓ In patients, a relationship was established between dimension "mobility" and dimensions "self-care" and "usual activities" from a quality of life test. Between "mobility" and "self-service" the rank estimate of correlation coefficient is a direct significant relationship (r=0.568). Relationship between "mobility" and "usual activities" is quite significant (r=0.610). Between "mobility" and "discomfort" is quite moderate (r=0.480).
✓ Between "self-care" and "daily activities" dimensions, the rank evaluation of correlation coefficient is a straight significant relationship (r=0.624). Between "self-care" and "discomfort" relationship is straight moderate (r=0.443). Between "habitual activities" and "discomfort" relationship is straight moderate (r=0.451).
✓ In patients, the relationship between "mobility" and "general health" is inversely significant (r=-0.520). Correlation between "mobility" and "health" is inversely significant (r=-600). Relationship between "self-care" and "health" is inversely moderate (r=-0.497). With a decrease in mobility, possibility of self-care and performing daily activities decreases. In the control group, relationship between dimension "mobility" and "self-care" is straight moderate (r=0.33, p<0 r=0.32,>
✓ Pearson's correlation coefficient was calculated (r=-0.492). Anxiety values increase, patients' health score decreases. Relationship between "anxiety" and "health rating" is inversely moderated. In control group, relationship between "anxiety" and "health assessment" is inversely weak (r=-0.155). Anxiety values increase, patients' health score decreases.
✓ Spearman's correlation coefficient was calculated between dimensions of quality of life and personality anxiety. Relationship between anxiety and investigated domains of quality of life is moderate: anxiety and mobility (r=0.481); between anxiety and self-care (r=0.390); between anxiety and daily activities (r=0.555); anxiety and discomfort (r=0.423). Higher scores for anxiety are reflected in increased problems in the examined dimensions of quality of life.
| anxiety | personality type D | general health | mobility | self service | usual activities | pain | |
| anxiety | 1.000 | 0.395 | -0.492 | 0.481 | 0.390 | 0.555 | 0.423 |
| personality type D | 1.000 | -0.221 | 0.233 | 0.267 | 0.251 | 0.332 | |
| general health | 1.000 | -0.520 | -0.497 | -0.600 | -0.386 | ||
| mobility | 1.000 | 0.568 | 0.600 | 0.480 | |||
| self service | 1.000 | 0.627 | 0.443 | ||||
| usual activities | 1.000 | 0.455 | |||||
| discomfort | 1.000 |
Table 16. Correlation coefficients of the influence of anxiety and type D personality on health and quality of life dimensions
✓ There is an inverse weak correlation between health assessment and type D personality in patients (r=-0.221). With higher values for personality type D, health score decreases. Relationship between dimension "negative affectivity" and health is inversely moderate (r=-0.464), and between the dimension "social isolation" and health is inversely weak (r=-0.224). As values for D personality expression increase, health score decreases. In controls, there was no relationship between health score and two D personality dimensions (P>0.01).
✓ A correlation was calculated between personality type D and anxiety in patients. Relationship is moderate (r=0.395). Between dimension "negative affectivity" of type D personality and anxiety, relationship is directly significant (r=0.685), and between dimension "social isolation" and anxiety (r=0.560). As D personality values increase, so does patient's level of anxiety. There is a weak correlation (r=0.259) between dimension "negative affectivity" and age of patients. With increasing age, values for this sphere also increase. Controls, no correlation was found between type D personality on both dimensions and anxiety (P>0.01).
Tested hypothesis about the factors that influence quality of life is confirmed. Anxiety and Type D personality are thought to be interrelated. Higher values of personality dimensions D influence the expression of personality anxiety. Anxiety and Type D personality have been hypothesized to negatively influence the health assessment and quality of life of COPD patients. Obtained results confirm the expectations that the stronger expression of dimensions "negative affectivity" and "social inhibition" are related to higher levels of personal anxiety. From the correlation analysis, it can be concluded that personal anxiety, negative affectivity and social isolation are interconnected in manifestations of personal factors leading to a change in quality of life of patients with COPD. Discussion of results highlighted issues related to impact of COPD on psychosocial sphere of patients' lives. Anxiety and limitations in physical activity are associated with manifestations of negative affectivity and social inhibition (personality type D). Outlined trends of personal and psycho-social manifestations are directly related to assessment of quality of life and have an impact on the spheres of life: physical activity; coping with daily activities; professional commitments; home and family care. Gender, place of residence and education do not influence the attitude towards healthy behavior (P>0.05). Place of residence was not a factor for better health awareness and ability to cope with daily problems related to the disease (χ2=9.45, p=0.15). Low physical activity was found in patients living in larger settlements, with secondary education and pensioners. There were significant differences in terms of active lifestyle between patients and controls. Personality predisposition is associated with higher levels of anxiety, difficulties in mobility, self-care, performing daily activities, and low self-esteem of personal health. Determinants of the quality of life in patients with COPD are: age, marital status, professional commitment, education, severity of main disease, personal characteristics. A lower self-assessment of quality of life is observed in elderly patients, unmarried, unemployed, with secondary education. Patients with higher education and professionally engaged are more responsible for their health, as well as people over 60 years old. Self-reported coping with work and family commitments was lower in patients. Problems in social life are expressed in limitations in communicating with family and friends, creating new social contacts, coping with routine activities, organizing daily life and other activities. Reduction of the main risk factors (smoking, low physical activity, etc.) leads to a reduction in morbidity. Results of pilot study confirm the influence of psycho-social factors on quality of life of patients with COPD. The analysis of the results for the quality of life and psycho-social risk factors leads to the differentiation of patients with a specific personality predisposition, low self-assessment of quality of life and problems in social adaptation. Research data show that patients have a high level of manifest anxiety.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
