
Research Article | DOI: https://doi.org/10.31579/2639-4162/067
1 Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands
2 MSc BSc RMN Lecturer in Mental Health Nursing with Dementia Specialty. University of Cumbria, Bowerham Road, Lancaster, LA1 3JD England.
*Corresponding Author: Jan van de Rakt, Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
Citation: Jan van de Rakt, Steve McCarthy-Grunwald (2022). Backward Falling Elderly. J. General Medicine and Clinical Practice. 5(3); DOI:10.31579/2639-4162/067
Copyright: © 2022 Jan van de Rakt, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 June 2022 | Accepted: 01 July 2022 | Published: 08 July 2022
Keywords: backward falling; balance; perception; pathological tone
Introduction
The investigation with video recordings through Prof. Robinovitch and colleague gave as outcome that backward falling was the most common fall accident in long car facilities.
Walking with an walking aid as an rollator frame gave no solution, elderly in long car facilities felt with this device also when the walk backward and often within three or four steps was the fall in progress.
Almost always was this an situation that was unstoppable and needed often the first assistance and/or supervision but forward walking was still good possible.
This great difference make us curious why walking backward was so risk full for falling.
Methods
An assessment was done by all people that has problems with backward walking but still walk good forward.
This population was very diverse. There were people out the long car facilities, nursing home residents but also elderly that live in their own house and about eighty precent has an diagnosis dementia.
The assessment contains investigation of the perception, the motoric reaction, balance reactions, tone and the selectivity.
Further one we search in the literature for investigation on this subject but also look at video captures how this fall take place and make an analyse.
Conclusion
The two elements that has the most impact were :
The stiffness of the trunk hip through pathological tone and/or hypertonus to maintain the attitude.
The perception under the feet with an direct relation with weight bearing but also the reaction of the balance system that was often not on right moment.
In 2017 published by K. van Schootenand their colleagues [1] an article that was an continuation of the famous article in the Lancet from Prof. DS. Robinovitch [2] and his group of investigators out 2012. That article was very important because now we could invest what the reason was that elderly fall and could this investigator group start with further assessment why this group of people fall.
Especially the group elderly with and without dementia and living in Nursing homes and/or long car facilities. Till than there were articles that try to assess [3] this problem but often they were limited, because they saw this people not fall.
That was an problem,because the method that was used, was asked this group elderly: “Why are you fallen ?” is often misunderstood and often was the person not capable to give an good answer. The answeris for everyone difficult, becauseoften is an fall an nasty experience and is the reasonfor the person not clear and then will the answer often an guess.
This periodhas consequences becausethe idea was then that there was an correlation directly with the disease especially dementia.
That there is an direct correlation exist between fall and neurological disease is obviousand that is also the case by people with dementia.
But often where the focus placed on the behavior component [4] and again that can be an reason, when peopleare afraid, wound upof in panic but again than is every elderlydangerous and not only elderly.
Than was the assumption that the cognitive element was greatest reason, that this group wasn’t capable to copy cognitive with the environment and that makes this group dangerous for falling. That older people with dementia frequenter almost two times, so often, but the problem isn’t not the cognitive aspect but the whole brain has an slower information processing.[5]
This slowerinformation processing and the investigation of the Robinovitch group is clear the greatest reason why elderlywith dementia fall often.
And specialbackward fallen is the greatest group. Out the investigation of K. van Schooten and others came the following data.
Direction of the fall in NursingHome [1] and whatwas the activity at the time of thefall.
Backward direction | 33.8 % |
Sideway | 28.8 % |
Straight down | 19.2 % |
Forward direction | 18.2 % |
Table 1: Activity at the time of the fall.
Walking | 33.6 % |
Standing | 24.0 % |
Stand to sit transfer | 17.5 % |
Sitting | 14.2 % |
Sit to stand transfer | 10.7 % |
Table 2
Incorrect weight transfer | 49.5 % |
Loss of support | 22.0 % |
Trip of stumble | 12.5 % |
Hit of bump | 8.8 % |
Table 3: is an continuation [1]. Common cause for fall in Nursing Home.
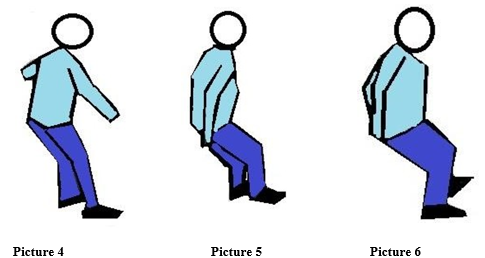
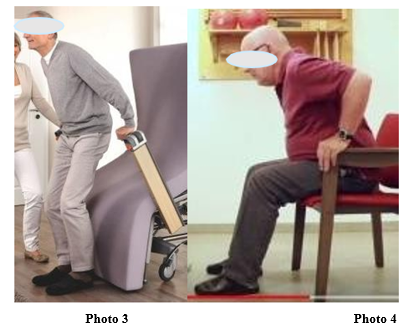
Back ward falling in pictures.
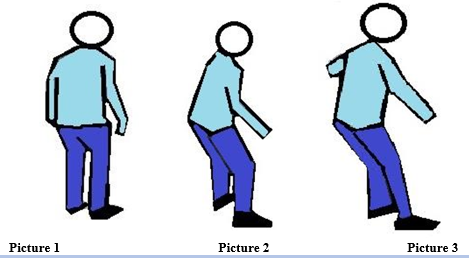
Normal balance reaction to the back.
Normal balance reaction for elderly is different that the balance reaction of younger people. Young people will, when they back walking often need only an simple reaction with the feet but elderly will need the feet and the trunk/hip reaction to brace the fall movement to the back.
Why this difference ? And is that still normal motoric ?
Become older is an process of adaptation. That means that elderly persons are busy continue with this adaptation and that will an body that is decreasing in all the functions that make balance optimal.
As the elderly let go things that he did before with his eyes closed than is that the sign that he knows that the risks that he can take are lesser.
Balance reaction is an reaction in which speed is an important issue and the amount of speed is decrease on all fronts and when we look how elderly move than is it clear that adaptation is going one.
It is important that therapist understand that balance problems is sign that the adaptation isn’t enough anymore and that the fall was there an important sign that the system has not the whole control.
To find the missing link why the fall risk is on that moment is greater than an period before is important and asked for an good assessment. Because the reason can be so divers and isn’t treatable with an simple training of balance and certainly people neurological disease as dementia.
Backward falling asked that elderly react with the feet and trunk/hip in his total.
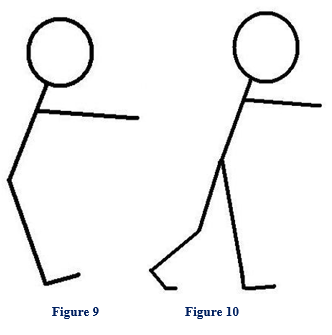
Balance reactions create time in which the shift of weight take place.
That shift must be complete because otherwise is the other leg not free and arises there the first problem to make an good step-strategy.
That free leg - step-strategy - must go far to the back.
The movement of the trunk/hip determinate the movement of the free leg. And this will be more extreme when the selectivity is lower.
Trunk/ hip- movements determinate the movements of the free leg !!
- Trunk/hip to the front, the free leg goes back.
- Trunk/hip to the back, the free leg goes to the front.
- Trunk/hip in elongation position, the free leg can cross
- Trunk/hip in shortening position, the free leg goes in abduction.
The power must be delivered through the pattern on the front side. That aren’t the strongest group but the have the capacity to react fast with an flexion in the hips/trunk and with an dorsal flexion in the feet
Loss of muscle power can therefore an reason that people cannot react on an disturbance in the front but still is it strange that only this would be the reason. Because an disturbance from the front is visible and by walking to the back would an relaxation of the trunk be possible.
of course an great loss of power would lead to an dominancy of the back but that is the question on his place that so many loss would inhibit all movements. Also standing up and walking.
Still this could be possible but in our belief not the most common reason. As cause we think on :
Ad.1. Loss of selectivity through loss of perception and therefore an less good input system. Awareness of movement under the foot and where the centrum of gravity exactly is.
Elderly with dementia have an perception system that often must participated with an worser input system. Till now it is this not certain what the reason is for this loss of input.
There are two possibilities and of course is there an third option that both elements are the cause :
1. Paratonia is an neurological form of tone increase as an answer of the damage brain in the cortical part. That makes that selectivity must be changed in more tone and the possibility to restrict the freedom[10] possibilities of the joint movements. But this tone increase, has an influence on the possibilities of the muscle spindles and that makes that this information is different and often far less selective. Thus tone-increase is an sign that the selectivity is lower and that the input is changed and less refined.
2. The other possibility is that the input system is of an lower quality. All senses are lesser and especially the movement feeling (discrimination-sense[10]) and recognition of the quality of the support ( gnostic sense[11]) are less by all elderly. But there is an rare element that especially elderly with dementia that are dependent in their movements, learned of this assistance and that changed the perception of the body. And that cognitive impairment has an influence on the body perception in the lying position in bed [12]. This will also occur in sit and standing position but there is no investigation on that area. Still there are signals that people that have assistance by the transfers that this changed their body perception in standing position. With support behind gave this people an signal that standing oblique to the back was in their perception right and the position right in our eye gave the feeling that they are falling to the front. The consequences of this changing of the body perception is that the balance reaction to the back get the signal in the brain later, even behind the heel and that will have an devastating result because everyone start to late.
Ad.2. Loss of selectivity through an pathological tone. By people with dementia is that paratonia.
This pathological tone is the answer of the damaged brain to control the movement through the synergies. But this synergies are movement pattern with an restricted amount of freedom degrees and that this means that selectivity is restricted.
The most important synergy for the balance is standing performance therefore the extension synergy.
That means that in the hip the tone of extension, endorotation and adduction is dominant. In the knee is that the extension.
And in the foot/ankle plantar flexion with inversion.
The muscle that take care for this synergy are the muscle that has the lowest selectivity and can work on the joint.
The adduction and endorotation of the hip will have an great impact but is necessary because this muscle can act for the hip and knee as an extensor and that is important because the selective extensor of hip and knee are not an part of the synergy pattern.
The feet are through this synergy vulnerable and asked for stability through shoes.
But the muscles that can place the hip in several positions, are through the dominancy of the muscles in the synergy inhibit.[17] Of course dependent of the loss of brain areas cortical.
The muscle that capable are for the great diversity, losses that power through the reciprocal inhibition of the dominancy of the muscle synergy pattern.
That means that walking with an straight spine and/or with an normal hip- and knee extension, because the synergy muscle pattern pull the leg in an adduction /endorotation with flexion in the hip and that count also for the knee.
This process is starting when the paratonia occur and will inhibit the speed that is necessary for an goof balance reaction.
One of the symptoms are that this person has difficult to walk straight because the hip extensor isn’t
so active anymore and this extension is done through the adductor muscle group.
When we see that knees are going to each other is that an sign that the synergy is dominant but in the time therefore is this paratonia present and asked much from that person.
The presence of paratonia and the synergy has for that person indirect the consequence that the trunk is often in an flexion position but with an great stiffness though the paratonia but also as an reaction on the synergy formation in the legs and that explains the immobility of the trunk that we say by people that walk backward as in the pictures 1-6.
Ad.3. Last part is that body perception to move sideways is changed and that this inhibit that the weight comes total on one leg.

Summary
Why is backward falling the most common fall by elderly and special elderly that live in long care facility or nursing home?
1. An great part of this people suffer from neurological diseases and that means that often the tone is pathological increase and makes balance difficult, but that higher tone is not alone present in the limb but also in the trunk and neck. The relaxation of the trunk muscles is almost impossible and replace this with an flexion in the hip is also difficult because here act the adductors as extensors.
2. But without an high pathological tone, elderly will often must have an higher normal tone in the spine to hold the trunk as erect as possible and that asked extra time to release that tone.
3. The perception is often changed through the caution and also walking with an aid as the rollator frame. The movement of the hip over the foot and under foot an restricted movement to the lateral. But by backward falling [18]is an extra perception deficit discovered but this is still an hypothetical why this occur. Elderly that walk backward and fall, let us every time the same process seen. Often three or four steps to the back, we see that the trunk is over the border of the back side of the heel. The strangest element is that this person give no balance reactions, not in the feet and not in the trunk. That whole balance reaction start much too late to give an proper step strategy, with as extra problem the stiffness of the trunk. The hypothetical part is why this balance reaction start to late.
Treatment or better slowing down this process!
1. Important is that the process of losing the perception of the body.
That means that there must be assessment what the possibilities are at that moment. That include the distal information senses as also the whole body perception through the use of the statiek technique. [19,20,21,23]. In the treatment-plan must that have an place from the day that especially standing up is difficult. Standing up by elderly is often done with using of the power of the arms. But when this power is required asked this for an upper trunk backward [6] and that will start the tonus increase in the back diagonals and makes this part of the trunk often more stiff. When this is the only way people can coming to stand and often accompanied with an assistance that stimulated this movement, will this further create only more stiffness and tonus increase in the upper trunk backward.
The lack of variation is one of the reason that the body perception changed and through the problem of the standing is the upper trunk always behind the feet and see we in the first period that the brain recognized that the balance isn’t good. After an period this signal is gone and that signal- dorsal flexion- is than active when the this people are falling and then there is not enough time to react.
When the push of the arms is dominant than will the placing of the feet often not totally occur. That because normal we flex in the hip to the front and without weight on the foot they were placed, where the belong.
But pushing with the arms or assistance on the arm stop this movement to early and that create an new learning moment in the brain but also an loss of independency

2. Mobility.
Restriction in the movement and especially in the joints are for elderly always an extra problem that asked for an adaptation. Back ward walking with an restriction in the trunk or/and the hips will asked much more from that person to hold the balance when he is walking backward. But despite this great problem, will elderly copy with this problem except when the perception and the tone are not normal.


3. Tonus hyper tonus of paratonia.
The tone is often not so high and when we assess than is this by an speed that we use by the measurement of the Mas-P according the Asworth scale. [27,28]
Often is the test on the arm elbow in sitting position normal. But that isn’t equal with the tone that people need to hold the standing position and walking /balance. There fore is it important to test also with more speed [28] and feel or the resistance changed. Test also the knee and feet movements.

When people are capable to walk and stand but have an slow balance reaction, than can an tone increase be an reason why the weight shift is an problem because this asked speed.
Is the test done with an tone that is zero or there is doubt or this tone is really zero, than increase the speed according the Tardieu scale [28]
When than an resistance occur than can this one of the reason why the balance is an problem.
Tone increase in the leg and arms will also an sign that the tone in the trunk is increase and that the synergy ( pathological ) has some dominancy. That means that this pattern will act dominant and that will make that the weight shift lateral is almost impossible and this group will walk with an rollator frame with an upper trunk sideway and with legs in adduction and endorotation.
There is another way to measure the tone and that is the Myotron-Pro. But the only prove we till today is that we measure the tone in stillness and not know what will occur when the speed increase. This last part will be an item that is important to assess by balance problems and also the symptoms occur by lot of people before the diagnosis Dementia is set. [30]
Important that the tone of the trunk muscle can we measured. That can we do in an sitting position through the placing technique [31]. Place your hand on the shoulder an give with the hand and verbal instruction that the person must flex the trunk so fast as possible an so far as possible. This cost some time but the reaction must be equal or faster that the time used in the Asworth scale.
This is often almost impossible because think everyone the mobility isn’t present.
Than test the mobility and tone after an period of rest lying on the back and then is often the relaxation present and is the movement easy.
Do the test than again but than in sitting position and often is than there all an difference and that is the pathological tone -paratonia or rigidity.
Especially the low tone differences that we assessed when we increase the speed, is the brace that the pathological tone will give by “fast “movements.
And this will also increase the tone of the trunk and an loss of selectivity in arms and legs but in an resting situation will nobody see what photo 13 let see.


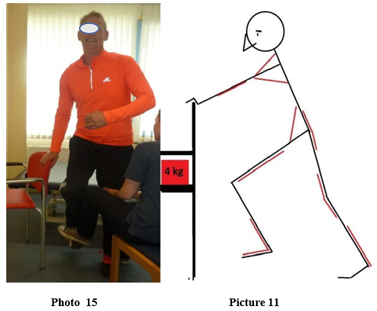
3. Shoulder position, compared this by the lady and by the gentlemen. The lady let the shoulder “hang” and there isn’t an high tone of the scapula. By the gentlemen is the opposite, no relaxation but together with tone increase of the trunk the shoulder blade are standing in retraction and this give in the gleno-humeral joint retroflexion and in the elbow an flexion. Sign that the tone is high in the trunk from cervical -thoracal -lumbar and this isn’t an “normal” high tone but here is an pathological tone active, necessary to hold control. Here we see the stiffness in the trunk that is so characteristic by backward falling.
4. The position of the hip and knee are signs that the legs must correct the attitude to hold the balance in this case not to fall to the back. And the lady is full in action on the end of their balance to the back. The white line let see how much of the body is for and back and the difference is great.
5. Feet action in by the gentlemen only an plantar flexion, maybe clawing in the toes and the exercise
was : “ Go so far as possible to the back”, this is the translation of the gentlemen.
The lady is on that endpoint and that seen we on the dorsal flexion in the feet.
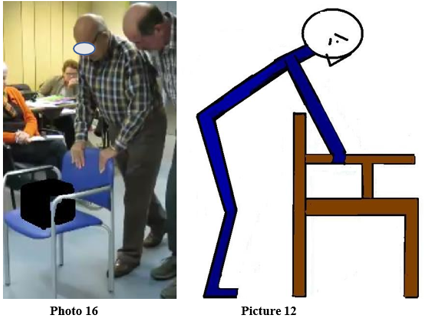
6. Looking to the performance together with the white line gives an clear picture what the problems are of the gentlemen. That is the high tone that makes it for him impossible to control the trunk despite the adaptation in the leg but the tone in the upper trunk is so high to brace the fall to the front and then is searching for an balance to the back very difficult and asked everything of the body perception because the tone will only increase.
The stretch on the muscles in the front part of the neck is high and that can together with the high tone give problems with eating and swallowing.[33]
4. Movement training walking and trunk /hip bending.
Often the moment that tone interfere with smoothly of the movements, is the moment that an walking aid or balance aid is necessary. Often is that the rollator frame and one of the greatest advance of this device that the necessity of an higher tone isn’t present.
But this device will decrease the power and coordination of the lower trunk and legs and almost always the lateral movement of the hip over the foot. That will change the perception and also the power that is present in the muscles around the hip.
The arms take an lot over but one of the movements that people not make, walking with an rollator frame, is bending through the arms and make more flexion in the trunk.
The moment that support is increasing on the arms the decrease of power and coordination in the legs go fast and this will increase the stiffness of the trunk.
This knowing must there an training program pointed on walking with an rollator in all direction and backward always with an more bending trunk.
Training of balance is of course important but when the tone is above Mas-P 1 than has this only useful when we can lowering the tone to get the necessary selectivity and that can only when the gravity is lowering (see point 7)
Training of the coordination and power must be done by task specific resistance training, that will give the best transfer and slow down the process.
Here we must care that the difficulty isn’t too high because that increase the tone.
We want movement against resistance within the possibilities of the person that increase the power and coordination.
We can this also do with walking behind an chair with resistance.
Pushing an chair with weight will change the posture totally from the attitude that people take when the walk behind the rollator frame.
The difference is that an chair with weight asked for an pushing action and walking with an rollator frame asked for an support on the handles to decrease the weight and coordination of the lower trunk and the legs.
Therefore pushing an chair is an treatment to slow the process.
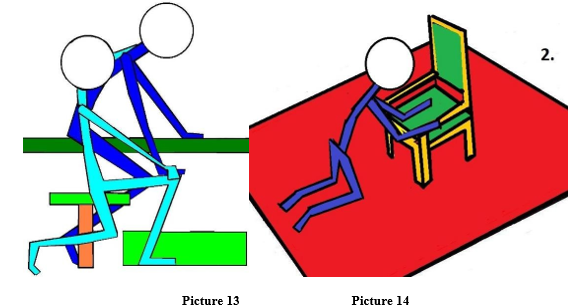
Resistance as photo 14 can be given in all directions, therefore with great variation and stimulated the standing leg to give stability and movement to sway the swing leg.
Bending the trunk and hip is possible with that chair but with much more attributes. With the chair is simple turning the chair and walk with this with an bending trunk. But to learn how the trunk to relax can be done by bending to the sit part, but also through lifting the chair of the floor and then placing and walking with the hands on the side support or even the sitting. of course is relaxation in sit and lying position also possible but the gravity is standing position is essential to get the feeling what relaxation is. Still this tone is an pathological tone and relaxation isn’t easy, stretch but also activation can give an decrease but also lowering of the gravity.
Pushing will activated an difference muscle pattern to get enough power from the trunk/legs to tha arms and get the chair in movement. Use load and calculated what the distance must be, how much rehearsal and the weekly frequency.
Muscle fatigue is an essential muscle stimulus to get an improving of the power and coordination of this muscle system.
5. Kneeling and standing up.
Elderly are afraid for falling but the reason isn’t only the pain but also the fact that the are afraid that
they are not capable to stand up and that they lie for hours on the floor.
This kneeling down or losing the back can be done when the person support himself with the hands/arms and legs, than is movements between this two point possible and that can decrease the tone and stiffness of the trunk.

That there are changing in the tone, in the muscle itself [33,34], in the joint of the spine but also the shoulder and hip is certain and all have influence on the tone and stiffness.
Prevention of backward falling will never be possible for everyone, but though the treatment will there be an lowering of the danger and the occurrence.
6. Perception under the whole foot.
Till today is by neurological diseases little effect found by training of the disturbed perception [35]. This comparing with the motoric approach was the conclusion that the motoric approach has an better effect also on the restoration of some body perception (total and local). At this moment is the activity the best perception treatment but by elderly with dementia is also damage in the cortical projections. The motoric performance will be alter through the tone and that will also have an influence on the body perception. Or is an lower perception the reason that the damaged brain seek for an solution and is that the use of pathological synergy with paratonia.
When we task specific resistance training apply with load will this also stimulated the perception of the body through the load will this give more body information in the brain.
Other alternative is water that gives through the hairs much more information that can influence the perception projection in the brain and that with an decrease tone.
7. Hydrotherapy.
The combination of the stiffness in the trunk/hip through the high tone and/or pathological tone (paratonia) and the restricted or even wrong body perception asked for an situation that can solve some of the problems.
Hydrotherapy can solve an few problems and create an environment that stimulated movement. This because moving in water give people an surrounding that support them and will brace the falls but has also an positive effect on the tone because the gravity is reduced [36].
This all together with an good program of balance training will give elderly with and without dementia the possibility to control the trunk/hip movement/mobility and will there help the weight bearing increase over the whole feet and will inhibit the “wrong “perception that we say when elderly start their balance to the back when the weight is passed the heel.
Backward falling is dangerous but on the other hand often present after an few steps to the back and can lead to trauma from legs, spine to the head.
Robinovitch team show that this occur the most in long car facilities and that this also occur with an walking aid.
We investigated what the reasons could be that caused this incapacity to walk back and not control the balance properly. This reasons were often and the stiffness of the trunk/hip and the body perception.
The awareness where the body is in totally but also where the weight on the feet were. By back ward falling was remarkable that the reaction occur often too late. When the weight was behind the heel than the reaction get starting and that is too late.
Further was the stiffness in the trunk/hip often high and was the reaction of the trunk to the front slow and that makes an step strategy no chance also because the trunk movement to the front facilitated the free leg to the back.
Still there are possibilities to slow down this process by an treatment that take care for trunk mobility and train the correct movement with an good perception.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
